Operationalizing Patient Safety at Academic Medical Centers
Chakraborti C, Kahn MJ, Krane K. Operationalizing Patient Safety at Academic Medical Centers. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2010.
Chakraborti C, Kahn MJ, Krane K. Operationalizing Patient Safety at Academic Medical Centers. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2010.
Perspective
Academic medical centers (AMCs) are complex organizations that deliver health care to the most severely ill and many uninsured patients.(1) They are also the site of most clinical education, significant amounts of research, and substantial innovations in both technology and delivery systems. Like all health care institutions, they have been challenged by the considerable data indicating large numbers of medical errors and quality defects in American medicine.(2) Recently, leaders of AMCs have taken up the mantle: a survey of medical center deans demonstrated that quality and patient safety are high priorities for their institutions.(3) In this report, we highlight the issues relevant to patient safety initiatives at AMCs.
Building the Culture
There is a clear consensus that transforming patient safety will require a substantial change in the culture of future clinicians. As the institutions that educate and train future physicians, AMCs have a unique opportunity to establish a culture of patient safety. Setting such a culture will require a commitment from senior leadership (4), along with faculty and staff with the requisite knowledge and skills in patient safety and quality improvement (PS/QI).(3-6) Some institutions will recruit such personnel, while others will create them by educating existing staff. Most, of course, will do some of each. Leaders will need to establish a fertile environment for such individuals by ensuring that PS/QI efforts will be "counted" for promotion and by developing an infrastructure that supports data gathering and publications. They can also help ensure a positive safety climate, one in which individuals are not blamed for innocent slips and mistakes.(7) Such an environment increases the probability that errors will be reported (8) and openly discussed.(9)
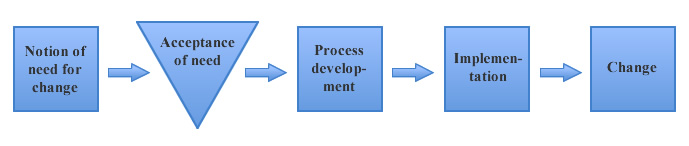
One significant barrier to patient safety is the need for cultural and organizational change.(10) Implementing change in an AMC is a multi-step process, which can be summarized by the process flow diagram illustrated in the Figure. In this diagram, tasks are indicated by squares and queues are indicated by inverted triangles. The major bottleneck in this process is the "acceptance" step—institutions that have created widespread acceptance of culture change appear to be the most successful in achieving safety goals.(11,12) Promoting change not only requires leadership and "cheerleading"—it also requires measurement to ensure that cultural goals are being met. Luckily, there are a number of validated instruments, such as the Safety Attitudes Questionnaire, that can accurately measure safety climate and ensure that interventions are having their intended effect.(12)
"You Can't Find a Fever If You Don't Take a Temperature"
Changing a culture ultimately requires changing the hearts and minds of individuals accustomed to "the way things have always been."(13) More persuasive strategies for change involve presenting the analyses of data that demonstrate change as necessary. Moving toward a culture of safety should be no different; but to advocate for change, AMCs need to obtain data that vividly illustrate the need for change through careful measurement tools. Additionally, hierarchies, prevalent in the department-dominated environment of most AMCs, reinforce a silo mentality. Structured communication tools such as situation-background-assessment-recommendation (SBAR) show promise in flattening hierarchies with minimal training.(14)
Awareness and Outreach
A small number of AMCs have succeeded in moving toward becoming highly reliable organizations.(15,16) Such organizations are characterized by strong leadership, commitment of resources, clear-cut accountability, and the development of safety champions.(17) While some made this change through strong leadership and commitment in the absence of substantial outside pressures, some have been driven toward transformation by being the site of highly public errors that generated tremendous pressure for change.(18-20) However, such change is certainly not universal among AMCs. Nor have many AMCs established partnerships with other organizations such as community hospitals and outpatient clinics. To establish a leadership role in the patient safety field, AMCs need to reach outside their walls to form multidisciplinary, multi-institutional collaboratives. Such collaboratives often include patients and their advocates, as well as health care professionals. Outreach of this kind emphasizes how AMCs embrace patient safety and promotes the kind of culture changes that are critical to safety improvements.
Pioneering Education
Academic medical centers are expected to model excellence in medical training. Incorporating patient safety into both the formal and informal curriculum has been encouraged since 2001 through the development of education programs for faculty, staff, and trainees.(5) While safety has been incorporated into organizational core competencies (21,22), the competencies that comprise patient safety remain unclear.
In 2004, the United Kingdom's Academy of Royal Medical Colleges presented a set of knowledge, skills, and attitudes as a blueprint for developing curricula geared toward patient safety and good medical quality.(23) In 2005, Australia developed a national safety education framework.(24) In late 2005, the American College of Surgeons described components of patient safety during a national consensus conference.(6) In reviewing these educational guidelines, several common elements are notable. First, learners must understand the nature of errors by identifying errors in their practices, and then analyzing and learning from these errors.
Second, trainees must improve their communication skills as they relate to discussion of medical mistakes. Improving general communication skills between health care providers and consumers is essential in medicine. However, like breaking bad news and engaging in end-of-life discussions, separate training may be needed in the specific communication skills involved in acknowledging errors and maintaining transparency in medicine.(8)
One of the key mental models of the patient safety field is that most errors are "system errors" committed by competent people working in dysfunctional systems. Therefore, a third educational competency is training students to understand basic quality improvement concepts, including fostering small, iterative, measurable changes to fix, assess, and re-assess problems (often called the plan-do-study-act [or PDSA] cycle).(25)
Another key discovery in the patient safety field was the large number of errors due to poor or absent teamwork. Therefore, a fourth competency is improved teamwork skills. Training in AMCs to improve teamwork skills may include mutual performance monitoring and backup support.(26) Since many AMCs train a number of disciplines, AMCs can provide a unique opportunity to promote teamwork by training physicians with other disciplines such as nurses, pharmacists, and social workers. In addition, such multidisciplinary training can be facilitated through the use of simulation to give trainees hands-on experience in advanced communication skills, teamwork, and real-time feedback and evaluation.(4,26)
Academic medical centers have always aimed to be the pinnacle of high-quality, innovative, state-of-the-art health care. However, until recently, most of their energy went into cutting-edge research and top-notch clinically oriented educational programs. The Institute of Medicine report on medical errors challenged AMCs to be leaders in providing safe care, performing the research needed to understand how to prevent mistakes, and training future generations of clinicians in the principles of patient safety. Most AMCs are working diligently to respond to this crucial challenge.
Chayan Chakraborti, MDAssistant Professor of Clinical Medicine Tulane University School of Medicine
Marc J. Kahn, MDProfessor of Medicine Senior Associate Dean for Admissions and Student Affairs Tulane University School of Medicine
N. Kevin Krane, MDProfessor of Medicine Vice Dean for Academic AffairsTulane University School of Medicine
References
1. Kohn LT. Academic Health Centers: Leading Change in the 21st Century. Washington, DC: National Academies Press; 2004. ISBN: 9780309088930.
2. Aspden P, Wolcott JA, Bootman JL, Cronenwett LR. Preventing Medication Errors: Quality Chasm Series. Washington, DC: National Academies Press; 2007. ISBN: 9780309101479.
3. Sachdeva AK, Philibert I, Leach DC, et al. Patient safety curriculum for surgical residency programs: results of a national consensus conference. Surgery. 2007;141:427-441. [go to PubMed]
4. Griner PF. Leadership strategies of medical school deans to promote quality and safety. Jt Comm J Qual Patient Saf. 2007;33:63-72. [go to PubMed]
5. Cottingham AH, Suchman AL, Litzelman DK, et al. Enhancing the informal curriculum of a medical school: a case study in organizational culture change. J Gen Intern Med. 2008;23:715-722.
6. Pratt SD, Mann S, Salisbury M, et al. John M. Eisenberg patient safety and quality awards. Impact of CRM-based training on obstetric outcomes and clinicians' patient safety attitudes. Jt Comm J Qual Patient Saf. 2007;33:720-725. [go to PubMed]
7. Leape LL, Woods DD, Hatlie MJ, Kizer KW, Schroeder SA, Lundberg GD. Promoting patient safety by preventing medical error. JAMA. 1998;280:1444-1447. [go to PubMed]
8. Gallagher TH, Waterman AD, Garbutt JM, et al. US and Canadian physicians' attitudes and experiences regarding disclosing errors to patients. Arch Intern Med. 2006;166:1605-1611. [go to PubMed]
9. Wachter RM, Shojania KG, Markowitz AJ, Smith M, Saint S. Quality grand rounds: the case for patient safety. Ann Intern Med. 2006;145:629-630. [go to PubMed]
10. Aspden P, Corrigan JM, Wolcott J, Erickson SM. Patient Safety: Achieving a New Standard for Care. Washington, DC: National Academies Press; 2004. ISBN: 9780309090773.
11. Mohr JJ, Batalden PB. Improving safety on the front lines: the role of clinical microsystems. Qual Saf Health Care. 2002;11:45-50. [go to PubMed]
12. Pronovost P, Sexton B. Assessing safety culture: guidelines and recommendations. Qual Saf Health Care. 2005;14:231-233. [go to PubMed]
13. Walton MM. Hierarchies: the Berlin wall of patient safety. Qual Saf Health Care. 2006;15:229-230. [go to PubMed]
14. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13(suppl 1):i85-i90. [go to PubMed]
15. Fitzmaurice J, Reardon G, Hopkins C, et al. Building a high reliability organization through a multi-method approach to monitoring the practice environment. In: Tartaglia R, Bagnara S, Bellandi T, Albolino S, eds. Healthcare Systems Ergonomics and Patient Safety. London, UK: Taylor & Francis Group; 2005:85. ISBN: 9780415377829.
16. Becoming a High Reliability Organization: Operational Advice for Hospital Leaders. Rockville, MD: Agency for Healthcare Research and Quality; 2008. AHRQ Publication No. 08-0022. [Available at]
17. Keroack MA, Youngberg BJ, Cerese JL, Krsek C, Prellwitz LW, Trevelyan EW. Organizational factors associated with high performance in quality and safety in academic medical centers. Acad Med. 2007;82:1178-1186. [go to PubMed]
18. Sachs BP. A 38-year-old woman with fetal loss and hysterectomy. JAMA. 2005;294:833-840. [go to PubMed]
19. Conway JB, Weingart SN. Organizational change in the face of highly public errors—I. The Dana-Farber Cancer Institute experience. [Perspective]. AHRQ WebM&M [serial online]. May 2005. [Available at]
20. The Josie King Foundation. Tony and Sorrel King. [Available at]
21. ACGME Outcome Project: Core Competencies. Chicago, IL: Accreditation Council for Graduate Medical Education; 1999.
22. AMA Initiative to Transform Medical Education. Chicago, IL: American Medical Association; 2005.
23. Wall D. Curriculum for the foundation years in postgraduate education and training. Med Teach. 2005;27:298-3016. [go to PubMed]
24. Walton MM, Shaw T, Barnet S, Ross J. Developing a national patient safety education framework for Australia. Qual Saf Health Care. 2006;15:437-442. [go to PubMed]
25. Boonyasai RT, Windish DM, Chakraborti C, Feldman LS, Rubin HR, Bass EB. Effectiveness of teaching quality improvement to clinicians: a systematic review. JAMA. 2007;298:1023-1037. [go to PubMed]
26. Chakraborti C, Boonyasai RT, Wright SM, Kern DE. A systematic review of teamwork training interventions in medical student and resident education. J Gen Intern Med. 2008;23:846-853. [go to PubMed]
Figure
Figure. Process flow diagram for implementing change in an academic medical center. (Go to figure citation in the text)![]()