All in the History
Case Objectives
- Describe the Emergency Medical Treatment and Active Labor Act (EMTALA) and understand that it does not apply to transfers to emergency departments from non-acute care facilities (e.g., nursing homes).
- Identify interventions to improve communication between referring facilities (such as nursing homes or clinics) and emergency departments.
- Describe what critical information should be conveyed during transitions in patient care in the emergency department.
- Appreciate how emergency physicians and inpatient physicians differ in their approach to patient diagnoses.
Case & Commentary: Part 1
A fatigued emergency department (ED) physician was coming to the end of his long shift when he was told there was a patient referral from an area nursing home. When he picked up the phone, the nursing home physician on the line started to explain, "I'm sending you a 68-year-old man with a history of interstitial lung disease who has been having some shortness of breath." At that moment, the call was interrupted as a senior nurse grabbed the ED physician and said, "We need you in code room one now!" The paramedics had just arrived in the ED with a critically ill patient.
The physician entered the room and found an elderly gentleman with no pulse, no blood pressure, and very low oxygen saturation. He began advanced life support—the patient was intubated and placed on mechanical ventilation, and given intravenous fluids, epinephrine, and atropine to treat his pulseless arrest. With this treatment, the patient regained a pulse and blood pressure after a few minutes but remained critically ill. Once the patient was somewhat stabilized, the ED physician searched for further information about the patient. The paramedics who had delivered the patient had left without speaking with him and did not leave any paperwork or documentation. The physician managed to find some papers with the patient that identified him as a 68-year-old nursing home resident with shortness of breath and included scant notes about medications, but no further information on past medical history. Only many hours later did the ED physician realize that this patient was the 68-year-old man that the nursing home physician had tried to sign out initially. Because of the interrupted signout and the inadequate handoff from the paramedics, the ED physician had no choice but to proceed with the evaluation and treatment of this patient despite minimal information.
The scenario faced by this emergency physician is all too common—because of lapses in communication, he was forced to make crucial medical decisions with little information. In this case, communication failures occurred between the nursing home and the ED as well as between emergency medical services (EMS) personnel and the ED. This case provides an opportunity to explore these critical transitions in care.
Although the majority of patients seen in EDs present directly or are brought by ambulance, many are referred from outside facilities such as other EDs, nursing homes, or local clinics (at our institution, this may be as high as 10% on a given day). These patients are frequently quite ill (which is often why they are referred in the first place) and may have already received significant medical evaluation or treatment prior to transfer. The Emergency Medical Treatment and Active Labor Act (EMTALA), enacted in 1986, was created to regulate some aspects of this referral process. EMTALA outlines specific expectations for both referring and receiving facilities to provide for safe transfer and to prevent the "dumping" of medically indigent patients who cannot afford to pay for their care (Table 1).(1,2) Unfortunately, EMTALA only applies to the transfer of patients to the ED from another ED, hospital, or medical center. The law does not apply to the referral of patients from non-acute care facilities such as nursing homes or clinics, and these transfers are not regulated in any systematic fashion. Thus, while it is a professional courtesy to contact EDs ahead of time about unstable (or stable) nursing facility patients, there is no legal requirement to do so.
Furthermore, there is no standardized protocol for this communication between providers (when it does occur). Two prior AHRQ WebM&M commentaries (3,4) highlight the frequency and hazards of signouts between medical providers for admitted patients in U.S. teaching hospitals (estimated at 1.6 million per year at UCSF alone).(5) The issues around the "signout" of patients referred to the ED are no different and should be subject to the same degree of oversight and standardization. The 2008 Joint Commission Patient Safety Goal 2E requires all health care providers to "implement a standardized approach to handoff communications" (6) and states that the organization's process for effective handoff communication ought to include (7):
- Interactive communication allowing opportunities for questions between the giver and receiver of patient information.
- Up-to-date information regarding patient condition, care, treatment, medications, services, and recent or anticipated changes.
- Methods to verify received information, including repeat-back or read-back techniques.
- Opportunities for the receiver to review relevant patient historical data, which may include previous care, treatment, or services.
- Limited interruptions to minimize the possibility that information fails to be conveyed or is forgotten.
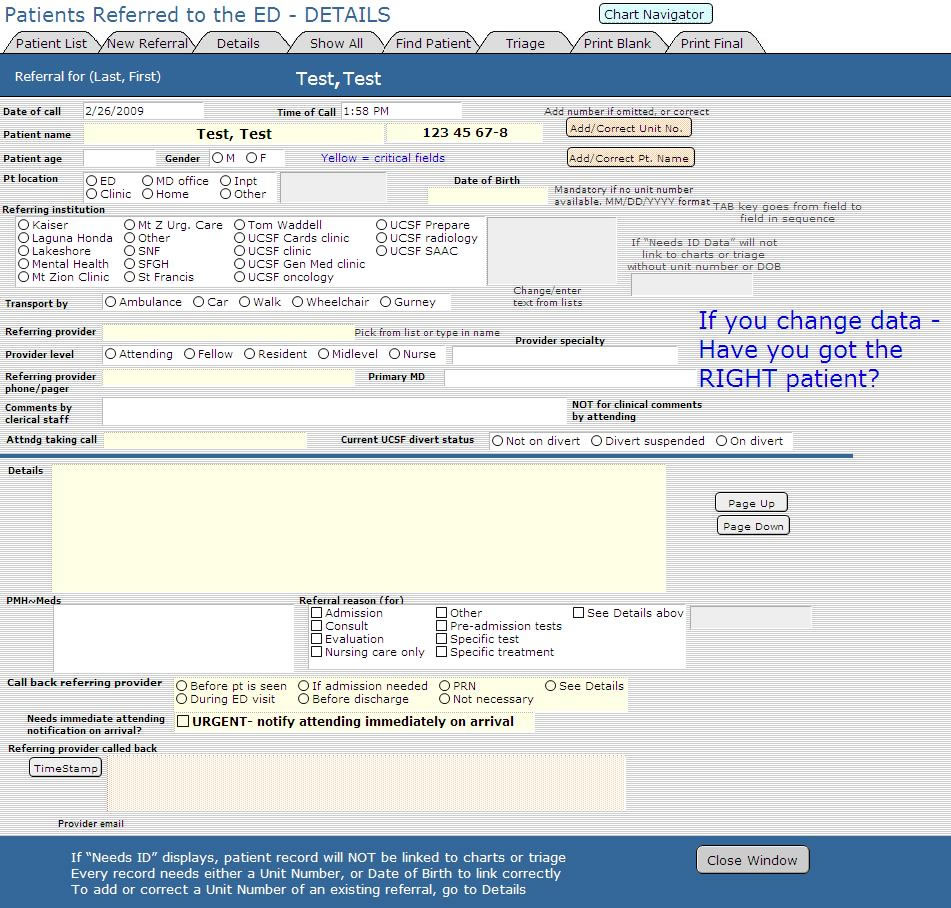
In a perfect world, referrals such as the one in this case would be communicated according to the Joint Commission guidelines. To start, the referral should occur prior to the patient's arrival to give the receiving ED physician an opportunity to ask questions. In reality, the referring provider is often consumed with providing emergent care (the reason for the transfer) and may not be free to discuss the transfer until EMS is en route to the ED, as in this case. Furthermore, the ED provider may be overwhelmed with multitasking (patient care or other administrative responsibilities) and thus may be unable to discuss the referral in adequate detail. Three simple interventions may ameliorate these inherent impediments. First, checklists (whether on paper or as part of an electronic medical record) can help the receiving facility and provider obtain crucial patient information. Examples of such checklists include an inpatient signout template highlighted in a previous AHRQ WebM&M commentary (4) or the UCSF ED referral template (Figure). Second, if coverage allows, dedicating an ED physician to manage administrative tasks, such as fielding referral calls, can allow an opportunity for more thorough exchange of information. Third, tasking administrative personnel with recording demographic data and referring provider information (most importantly, a call back number) might reduce the time required of the ED provider, who can then concentrate primarily on the essential medical information.
Another weak communication link in the ED highlighted by this case can occur at the transfer of care between EMS and the ED. Many health care systems require EMS providers to radio the receiving ED prior to arrival. These "ring downs" are necessarily brief, do not include identifying information (beyond patient age and gender, due to the insecure nature of radio communication), and are often complicated by poor reception. Thus, a formal face-to-face report is preferred. EMS providers must transfer care to a provider with a higher scope of practice, most often a registered nurse. In the case of an unstable patient, as determined by the EMS providers or by the triage nurse, EMS providers often report directly to the ED physician. This official report, whether to the nurse or the physician, generally includes the patient's chief complaint and history, pertinent physical examination findings including vitals, and any response to prehospital treatment. But note that there is no national standard for this process. Moreover, in practicality, this direct verbal communication can be challenging. In the case of an unstable patient, there may be a cacophony created by multiple providers in the resuscitation room (physicians; nurses; respiratory therapy; radiology technicians; pharmacy, laboratory, and blood bank personnel, etc.), all of whom have crucial roles to play. Ideally, the room should be quiet with the exception of the reporting EMS provider and receiving physician, with all other personnel diligently performing their preestablished tasks. However, anyone who has been present during resuscitations knows that this is the exception.
EMS "runsheets" (EMS provider documentation of the patient encounter) are designed to include these data in a succinct written format (whether paper or electronic). However, EMS documentation is often incomplete upon arrival due to patient acuity and time constraints. A recent report from a suburban academic ED revealed that EMS personnel verbally relayed only 44% of pertinent data contained on their runsheets.(8) Some systems require the ED nurse or physician to sign the EMS runsheet acknowledging the transfer of care. Although forcing a signature may not improve the timely completion of the runsheet or ensure direct communication, it may force the accepting providers to review the information (even if later), and hospitals should consider making this a standard policy. Simply leaving the patient on an ED gurney does not constitute an appropriate transfer of care and may be considered patient abandonment.
Case & Commentary: Part 2
A stat chest radiograph revealed infiltrates in the left lung. Based on the minimal information at hand (the history of shortness of breath, the low oxygen levels, the cardiac arrest, and the chest x-ray), the ED physician made a presumed diagnosis of aspiration pneumonia with respiratory arrest and septic shock. The patient was given intravenous antibiotics, fluids, and vasopressors for blood pressure support. The ED physician contacted the intensive care unit (ICU) team who would be managing the patient in the ICU. He remained busy with this patient (and others in the ED) and could only give a brief signout: "He is a 68-year-old man with a possible history of lung disease with probable aspiration pneumonia. He's intubated, on pressors, and has already received antibiotics. He needs to get up to the ICU." At that moment, another patient was crashing and the physician had to hang up.
The admitting ICU team evaluated the patient and agreed with the initial assessment (although they were concerned by the limited information available). The patient was taken to the ICU. Three hours later, the patient had another arrest, becoming pulseless without a blood pressure. After being treated with aggressive fluids and three vasopressor medications, his blood pressure remained low.
At this point, the puzzled admitting team contacted the nursing home physician. Further history revealed that the patient's shortness of breath had been very acute in onset and had been associated with chest pain, and the patient had stated at the time that he "felt faint and like he was going to die." Based on this vital piece of information, the team became concerned that a pulmonary embolism (blood clot to the lungs) was the cause for his critical illness. The patient was treated with thrombolytics (clot-busters) for presumed massive pulmonary embolism 5 hours after he arrived at the hospital.
The patient immediately responded to treatment, with improvements in his oxygen level and blood pressure. He continued to improve and, after a prolonged hospitalization, ultimately returned to the nursing home.
The transition in care (handoff) between the ED and the inpatient providers creates an opportunity for communication breakdown and medical errors. As with all transfers of care, this should be done in accordance with the 2008 Patient Safety Goal 2E guidelines.(6) Based on clinical experience, most providers feel that the ED physician's presentation to the admitting team should be brief but thorough and include the items listed in Table 2. Contact information for referring providers, if available, should be conveyed. This process should last no longer than a few minutes and normally takes place in the form of a brief phone conversation, though a face-to-face conversation is preferable. In the case of critically ill patients, this process is best accomplished in person at the patient's bedside.
In a recent survey of emergency and internal medicine providers from a large academic medical center, 29% of respondents reported that a patient of theirs had experienced an adverse event or near miss after ED to inpatient transfer.(9) The most common etiologies for these events were errors in diagnosis, treatment, and disposition. Respondents identified numerous contributing factors including inaccurate or incomplete information (particularly vital signs); ED crowding; high workload; difficulty in accessing key information such as vital signs, pending data, ED notes, ED orders, and identity of responsible physician; nonlinear patient flow; "boarding" in the ED; and ambiguous responsibility for signout or follow-up.(9) Potential solutions include improved electronic access to key information (such as vital signs, ED notes and orders, laboratory and radiology studies, and pending studies), and signout checklists (Table 2). Although the ED physician in this case was not aware of the key aspects of the history from the nursing home, a more standardized, clear, and pertinent signout could have improved the care of the patient.
One additional contributor is particularly noteworthy: cultural differences and misunderstandings, especially around roles in determining the final diagnosis. Emergency department diagnoses are often uncertain at best (due to patient acuity, limited interaction, incomplete laboratory/radiographic data, and limited time to assess response to therapies). This uncertainty may not be appreciated by admitting teams and may be related to ED physicians overstating confidence in their diagnoses (a need to "prove" that the patient requires admission [9]), or because of clinical inertia (failure of health care providers to initiate or intensify therapy when indicated) or cognitive biases (the tendency to make errors in judgment based on cognitive factors). A colleague of mine has said that ED physicians are "sensitive," while admitting teams aim to be "specific" (i.e., the emergency physician's role is to stabilize the patient and determine appropriate disposition, not definitively diagnose or manage their care). This cultural chasm can contribute to admitting teams' mistrust of ED ability, judgment, or professionalism, thus creating further barriers to effective communication.
A consequence of admitting teams not fully appreciating the ED approach to establishing the diagnosis is premature closure. Premature closure is the tendency to stop considering other possible diagnoses after a diagnosis is reached.(10) The ED physician can help to avoid this phenomenon by acknowledging diagnostic uncertainty and simply referring to the patient's complaints as the final ED diagnosis and suggesting a differential diagnosis (e.g., "respiratory failure of unclear etiology, possible aspiration vs. community-acquired pneumonia vs. pulmonary embolism, etc.") rather than labeling the patient with a definitive diagnosis (e.g., aspiration pneumonia). The internist, on the other hand, can avoid this cognitive trap by making a conscious effort not to accept a diagnosis as definitive after reaching (or being given) one, but to ask "What alternatives should be considered?" This should be done initially and intermittently as the clinical case evolves. Diagnoses may seem obvious initially, but time is often our best diagnostic tool, and this simple mental back-up mechanism can help to avoid errors. In this case, the admitting team may have initially "anchored" on the diagnosis provided by the ED, which potentially delayed receipt of the definitive appropriate therapy.
This case illustrates many potential pitfalls in signouts, whether they be from a nursing facility to an ED, EMS to ED, or ED to admitting team. Playing "telephone" is great fun as a child, but when lives are at stake, it is anything but humorous.
Take-Home Points
- Transitions of care in the ED should follow the Joint Commission standardized guidelines for effective handoff communications.
- Emergency departments should employ checklists (either paper or digital) to improve transitions of care from referring facilities.
- Emergency medical services personnel should be required to provide a direct verbal signout to ED providers as well as a written report ("runsheet").
- The handoff between the ED and inpatient teams should be brief but standardized to include the pertinent clinical information.
- Emergency physicians and inpatient services approach final diagnoses in different ways, and this cultural divide can lead to errors and poor patient outcomes. Both groups should strive to understand and appreciate the other's perspective.
Christopher Fee, MD Assistant Clinical Professor of Emergency Medicine University of California, San Francisco, Medical Center
Faculty Disclosure: Dr. Fee has declared that neither he, nor any immediate member of his family, has a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, his commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. Emergency Medical Treatment and Active Labor Act (EMTALA) overview. Centers for Medicare & Medicaid Services. [Available at]
2. EMTALA. American College of Emergency Physicians. [Available at]
3. Vidyarthi A. Fumbled handoff. AHRQ WebM&M [serial online]. March 2004. [Available at]
4. Vidyarthi AR. Triple handoff [Spotlight]. AHRQ WebM&M [serial online]. September 2006. [Available at]
5. Vidyarthi AR, Arora V, Schnipper JL, Wall SD, Wachter RM. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1:257-266. [Available at]
6. 2008 National Patient Safety Goals Hospital Program. The Joint Commission. [Available at]
7. The Joint Commission Accreditation Program: Ambulatory Health Care National Patient Safety Goals. [Available at]
8. Benner JP, Hilton J, Carr G, et al. Information transfer from prehospital to ED health care providers. Am J Emerg Med. 2008;26:233-235. [go to PubMed]
9. Horwitz LI, Meredith T, Schuur JD, Shah NR, Kulkarni RG, Jenq GY. Dropping the baton: a qualitative analysis of failures during the transition from emergency department to inpatient care. Ann Emerg Med. 2009;53:701-710. [go to PubMed]
10. Redelmeier DA. Improving patient care. The cognitive psychology of missed diagnoses. Ann Intern Med. 2005;142:115-120. [go to PubMed]
Tables
Table 1. Emergency Medical Treatment and Active Labor Act (EMTALA) Expectations for Transferring and Receiving Facilities.(2)
Transferring facilities are obligated to:
|
Table 2.
During the transition in care, verbal signout from ED providers to inpatient providers should include:
|
Figure
Figure. UCSF Emergency Department Referral Template.