A Pill Organizing Plight
McGalliard B, Shane R, Rosen S. A Pill Organizing Plight. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2016.
McGalliard B, Shane R, Rosen S. A Pill Organizing Plight. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2016.
Case Objectives
- Identify patients at high risk for adverse drug events.
- List drugs that are considered inappropriate in older patients.
- Describe best practices for medication reconciliation.
- Provide strategies to improve medication management in geriatric patients.
The Case
As part of an outpatient geriatrics rotation, an internal medicine resident visited one of his patients—an 80-year-old, Spanish-speaking woman with multiple medical problems including hypertension, hypothyroidism, hyperlipidemia, gastroesophageal reflux, coronary artery disease, and depression—in her home for recent onset of lightheadedness and dizziness. At a recent outpatient visit, she had been diagnosed with Alzheimer dementia for which she was prescribed a new medication, donepezil. Her family was advised that she would require ongoing assistance to manage complex tasks including organizing her medications.
During the home visit, the resident reviewed the patient's medications in detail. The patient's medical record revealed that she was supposed to be taking eight medications daily, including losartan and hydrochlorothiazide for hypertension, levothyroxine for hypothyroidism, pantoprazole for gastroesophageal reflux, aspirin for coronary artery disease, simvastatin for hyperlipidemia, escitalopram for depression, and the newly prescribed donepezil.
The patient reported using a pillbox, which her daughter sometimes filled for her when she visited. The resident identified several errors in the pill organization system, including empty slots for upcoming days as well as slots that contained a higher number of blood pressure medications than the patient was supposed to take. The resident also discovered that an old blood pressure medication (a beta-blocker), which had been stopped by the patient's cardiologist months ago, was still in the pillbox. As a result of these problems, on some days the patient was taking up to five blood pressure pills when she was only supposed to be taking two. The resident suspected that her symptoms of lightheadedness and dizziness were the result of intermittently overdosing on blood pressure medications. Additionally, the resident discovered that the new medication—donepezil—was not in any of the pill slots because the patient's daughter was unaware that it had been prescribed to the patient and therefore never picked it up from the pharmacy.
Fortunately, the resident was able to spend time explaining the clinical significance of each medication to the patient's daughter and helped her develop a standard approach to filling her mother's pillbox each month. A follow-up home visit revealed that once the pillbox had been properly organized, the patient's lightheadedness and dizziness had resolved.
The Commentary
by Brittany McGalliard, PharmD; Rita Shane, PharmD; and Sonja Rosen, MD
This case illustrates how two seemingly simple medication errors—failure to stop the beta-blocker and the delay in initiation of donepezil—resulted from the complexities associated with medication management in an older and non–English-speaking patient. This case presents an opportunity to broadly outline best practices for reducing adverse drug events (ADEs) across transitions of care.
Age-associated changes in body composition, metabolism, and pharmacodynamics make drug–drug and drug–disease interactions problematic for older adults, placing them at increased risk for delirium, falls, and other adverse outcomes including hospital readmission. Patient-specific risk factors for adverse outcomes include patients with multiple comorbidities and those identified as frail.(1) Polypharmacy, generally defined as the prescription of five or more medications, is common in older patients and is often associated with adverse drug reactions, more frequent hospitalization, and increased morbidity.(2) Poor patient record-keeping, renal insufficiency, the use of multiple pharmacies, and having more than one prescriber may increase the risk of ADEs by as much as 30% (Table).(3,4) When providers are unable to effectively communicate with patients or caregivers due to language barriers, rates of adverse events are also increased.(5) Additionally, patients with cognitive impairment are at higher risk for confusion regarding their medication regimen than those without such impairment.(6,7) Therefore, every encounter with an older patient—especially at the time of a care transition (e.g., hospital discharge)—presents an opportunity to reduce the total number of medications prescribed to only those that are necessary.(8)
A number of resources exist to support clinicians in reducing ADEs.(9) Criteria have been developed for medication selection in frail patients along with recommendations for patients with delirium and dementia.(10) Both the Beers Criteria and STOPP (Screening Tool of Older Persons' potentially inappropriate Prescriptions) Criteria provide lists of medications that should be avoided in the geriatric population.(11,12) The updated 2015 Beers Criteria includes information on significant drug–drug interactions, medications that should be avoided or require adjustment in patients with renal dysfunction, and the use of antipsychotics for patients with behavioral problems. It also recommends stopping proton pump inhibitors after an 8-week course.(13) A recent study comparing two older versions of the Beers with the STOPP Criteria demonstrated that all three were modestly prognostic for ADEs, emergency department visits, and hospitalizations, with the STOPP Criteria slightly outperforming both earlier versions of the Beers Criteria.(14)
Best Practices for Medication Reconciliation
Accurate medication reconciliation—the process by which a patient's most accurate medication list is determined, documented, and communicated among providers and patients—can enhance patient safety by mitigating drug discrepancies across the continuum of care. For example, medication changes made during a hospitalization may need to be reversed or further altered at the time of hospital discharge.(15) One study demonstrated that at least one medication inaccuracy was identified in 46% of prior-to-admission medication lists in older patients.(16) In 2006, The Joint Commission issued a Sentinel Event Alert recommending that medication reconciliation be performed at every care transition—including when patients are transferred between practice settings, specialties, and levels of care—to avoid errors.(17) The first step in the process of medication reconciliation includes an accurate medication history, which needs to be updated at each health care encounter as well as every time a medication is initiated, changed, or discontinued. This includes prescription and nonprescription medications as well as supplements. These lists should be considered "living documents" that may change frequently and should be updated as such.
In physicians' offices, medical assistants are often responsible for updating the medication list in electronic health records. To prevent patient harm, a protocol for "Universal Precautions for Medication Lists" has been developed and underscores the importance of verifying the medication list for accuracy at each encounter.(18) The use of previsit medication questionnaires has been shown to significantly reduce the number of medication discrepancies.(19) Patients should be instructed to request an updated medication list each time they obtain prescriptions from their pharmacies. Additionally, pharmacist-led brown bag medication reviews can identify significant drug-related problems, increase patient satisfaction, and augment patient understanding of medication regimens.(20,21) Non–English-speaking patients may require use of translators and translated educational materials as well the presence of an interpreter during discussion of medications with a provider.(22)
Errors on admission medication lists are problematic and can lead to errors during hospitalization and after discharge. A recent randomized control trial evaluating the accuracy of medication histories obtained in the emergency department in high-risk patients found that standard medication histories were associated with 7.4 medication errors per patient. This rate fell to 1.4 errors per patient when the histories were obtained by a pharmacist or trained pharmacy technician.(23) Pharmacy claims data available through some electronic health records can also be used to increase the accuracy of the medication list.(24)
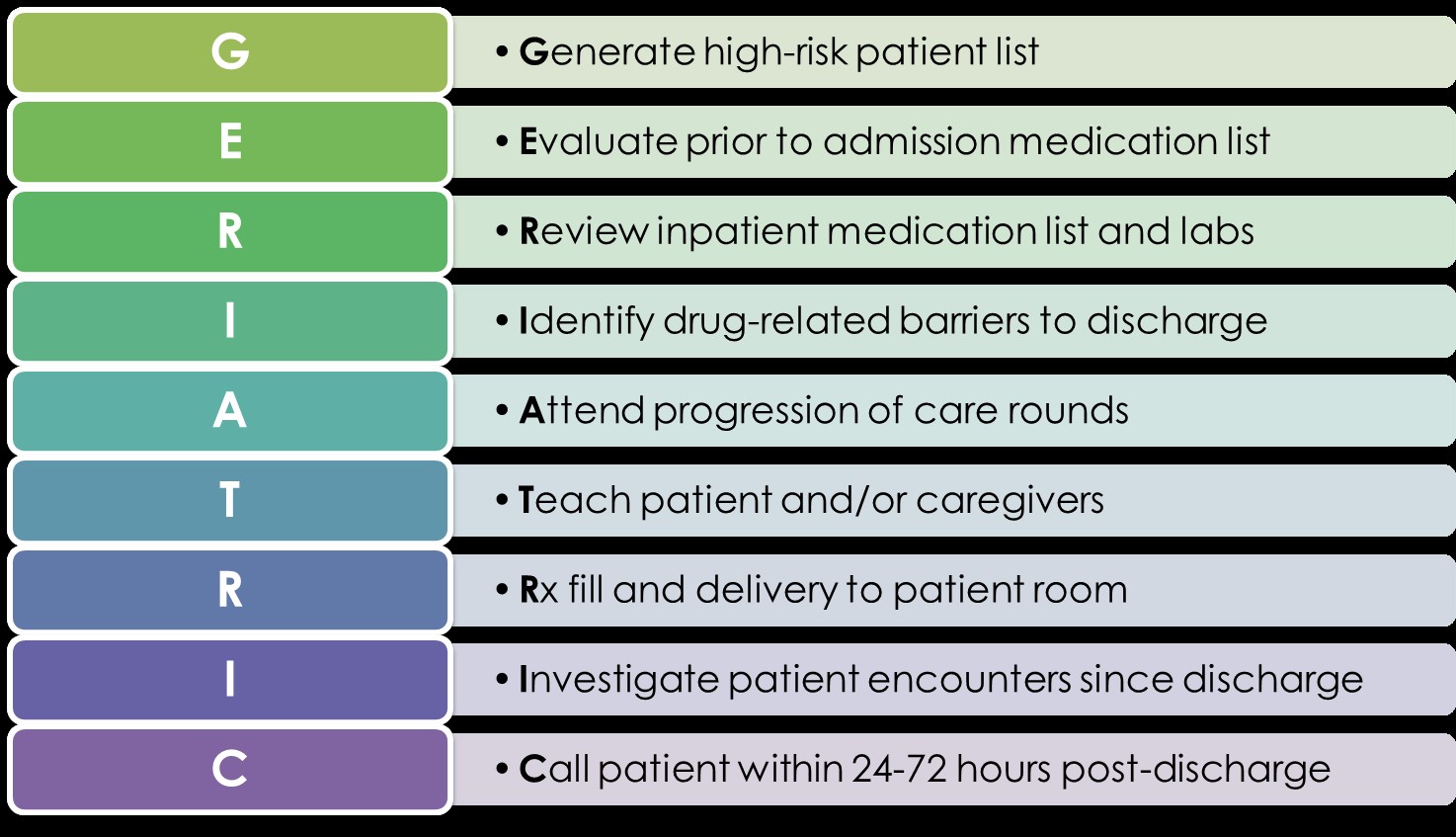
Pharmacists play a key role in medication reconciliation, education, and postdischarge follow-up to ensure safe medication use after hospitalization. Evidence demonstrates that pharmacist involvement leads to reductions in ADEs and readmissions of 30% or greater.(25,26) Recently, a UCLA Medical Center pharmacy pilot demonstrated a 56% decrease in all-cause 30-day readmission rates and a 90% reduction in medication-related readmissions on a geriatric special care unit. In this study, a dedicated pharmacist performed medication reconciliation both after admission and before discharge, daily medication review, predischarge bedside counseling, and a follow-up phone call within 48 hours to identify and resolve medication-related problems and triage clinical issues to the appropriate health care provider.(27) The GERIATRIC method provides a stepwise approach to addressing important medication issues at transitions of care (Figure). Preliminary results using this method demonstrated that opportunities exist to improve medication use in 82% of patients.(28)
Home health visits, as illustrated in this case, or virtual visits, are valuable for assessing the patient's environment, support systems, and prescriptions. In addition, they may help to identify errors and prevent harm. Patients often have previously discontinued medications at home, as exemplified by the beta-blocker in this case. Patients with cognitive impairment may be at higher risk for continuing discontinued medications, potentially resulting in ADEs.(29,30) For patients admitted to long-term care and skilled nursing facilities, consultant pharmacists should reconcile the medications ordered with the prior-to-admission medication list to make sure there are no discrepancies.
Recommendations for Medication Management
Resources to improve prescribing safety in older patients include the STOPP list, the American Geriatrics Society Choosing Wisely list, and recommendations for pharmacy's role in Choosing Wisely.(31) Choosing Wisely is designed to reduce overuse of treatments and procedures based on evidence that these lead to more harm than benefit.(12,32) Evidence supports the effectiveness of geriatric specialists in decreasing the rate of inappropriate prescribing practices; one study found a 35% decrease in outpatient ADEs.(33) Geriatricians are attuned to the dynamic pathophysiological and psychosocial processes associated with aging, and outpatient geriatric interventions result in a significant reduction in the number of medications prescribed to older patients as well as in the number of hospitalizations and the cost of medications and overall health care.(34-38) In addition, a single prescriber should be responsible for prescribing all medications for an individual patient to decrease potential for ADEs.
Periodic evaluation of medications by pharmacists can also identify opportunities to simplify the regimen, provide patient education, and assess adherence is recommended. Providing patients with a medication calendar that includes the times of day to take medications can reduce confusion about which medications to take when. The calendar can also be used to record when the medications were taken to reduce omitted or extra doses. Organizing medications in a pillbox as was done in this case facilitates adherence to the prescribed regimen. Medication access interventions, including unit dose packaging, have demonstrated an increase in medication adherence in older patients but may not be appropriate for some patients due to cost or physical limitations.(38)
Take-Home Points
- Medication reconciliation is essential at every encounter and care transition.
- Avoid potentially inappropriate drugs in older patients.
- A single prescriber should be responsible for prescribing all medications for an individual patient to reduce potential for adverse drug events.
- Adhere to Choosing Wisely recommendations supported by the American Geriatrics Society and the American Journal of Health-System Pharmacy.
- Implement predischarge medication reconciliation and education with a structured postdischarge follow-up call using a standardized checklist.
Brittany McGalliard, PharmD Post-Graduate Pharmacy Resident Cedars-Sinai Medical Center
Rita Shane, PharmD Chief Pharmacy Officer Cedars-Sinai Medical Center Assistant Dean Clinical Pharmacy UCSF School of Pharmacy
Sonja Rosen, MD Geriatric Specialist Cedars-Sinai Medical Center
Faculty Disclosure: Drs. McGalliard, Shane, and Rosen have declared that neither they, nor any immediate members of their families, have a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, the commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. Sternberg SA, Wershof Schwartz A, Karunananthan S, Bergman H, Clarfield AM. The identification of frailty: a systematic literature review. J Am Geriatr Soc. 2011;59:2129-2138. [go to PubMed]
2. Maher RL, Hanlon JT, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13:57-65. [go to PubMed]
3. Rosen S, Mariano J. Geriatric principles. In: Chun A, Schwartzberg JG, Irmiter C, eds. Geriatric Care By Design: A Clinician's Handbook to Meet the Needs of Older Adults Through Environmental and Practice Redesign. 1st ed. American Medical Association Press; 2011. ISBN: 9781603596589.
4. Pretorius RW, Gataric G, Swedlund SK, Miller JR. Reducing the risk of adverse drug events in older adults. Am Fam Physician. 2013;87:331-336. [go to PubMed]
5. Wilson E, Chen AH, Grumbach K, Wang F, Fernandez A. Effects of limited English proficiency and physician language on health care comprehension. J Gen Intern Med. 2005;20:800-806. [go to PubMed]
6. Alsaeed D, Jamieson E, Gul MO, Smith FJ. Challenges to optimal medicines use in people living with dementia and their caregivers: a literature review. Int J Pharm. 2016;512:396-404. [go to PubMed]
7. Gray SL, Mahoney JE, Blough DK. Adverse drug events in elderly patients receiving home health services following hospital discharge. Ann Pharmacother. 1999;33:1147-1153. [go to PubMed]
8. Reuben DB, Rosen S. Principles of Geriatric Assessment. In: Hazzard's Geriatric Medicine and Gerontology. Halter JB, Ouslander JG, et al, eds. 6th ed. McGraw Hill Education; 2009. ISBN: 9780071488723.
9. Adverse drug events in older adults: how to avoid them. Am Fam Physician. 2013;87. [go to PubMed]
10. Huisman-Baron M, van der Veen L, Jansen PA, van Roon EN, Brouwers JR, van Marum RJ. Criteria for drug selection in frail elderly persons. Drugs Aging. 2011;28:391-402. [go to PubMed]
11. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63:2227-2246. [go to PubMed]
12. Gallagher P, Ryan C, Byrne S, Kennedy J, O'Mahony D. STOPP (Screening Tool of Older Person's Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment): consensus validation. Int J Clin Pharmacol Ther. 2008;46:72-83. [go to PubMed]
13. Trucil D. Expanded AGS Beers criteria offer new guidance, tools for safer medication use among older adults. New York, NY: The American Geriatrics Society; October 8, 2015. [Available at]
14. Brown JD, Hutchison LC, Li C, Painter JT, Martin BC. Predictive validity of the Beers and Screening Tool of Older Persons' potentially inappropriate Prescriptions (STOPP) Criteria to detect adverse drug events, hospitalizations, and emergency department visits in the United States. J Am Geriatr Soc. 2016;64:22-30. [go to PubMed]
15. Shekelle PG, Pronovost PJ, Wachter RM, et al. The top patient safety strategies that can be encouraged for adoption now. Ann Intern Med. 2013;158:365-368. [go to PubMed]
16. Bahrani L, Eriksson T, Höglund P, Midlöv P. The rate and nature of medication errors among elderly upon admission to hospital after implementation of clinical pharmacist-led medication reconciliation. Eur J Hosp Pharm. 2014;21:156-160. [Available at]
17. Using medication reconciliation to prevent errors. The Joint Commission. Sentinel Event Alert. January 25, 2006;(35):1-4. [Available at]
18. Shane R. Why 'Universal Precautions' are needed for medication lists. BMJ Qual Saf. 2016;25:731-732. [go to PubMed]
19. Tattersall C, Hartry N, Ram AR. Improving the accuracy of medication history taking in a diabetic eye clinic. Br J Nurs. 2008;17:598-600. [go to PubMed]
20. O'Connell MB, Chang F, Tocco A, et al. Drug-related-problem outcomes and program satisfaction from a comprehensive brown bag medication review. J Am Geriatr Soc. 2015;63:1900-1905. [go to PubMed]
21. Sarzynski EM, Luz CC, Zhou S, Rios-Bedoya CF. Medication reconciliation in an outpatient geriatrics clinic: does accuracy improve if patients "brown bag" their medications for appointments? J Am Geriatr Soc. 2014;62:567-569. [go to PubMed]
22. Blennerhassett J, Hilbers J. Medicine management in older people from non-English speaking backgrounds. J Pharm Pract Res. 2011;41:33-36. [Available at]
23. Pevnick JM, Nguyen CB, Jackevicius CA, et al. Minimizing medication histories errors for patients admitted to the hospital through the emergency department: a three-arm pragmatic randomized controlled trial of adding admission medication history interviews by pharmacists or pharmacist-supervised pharmacy technicians to usual care. J Patient-Centered Res Rev. 2015;2:93. [Available at]
24. Phansalkar S, Her QL, Tucker AD, et al. Impact of incorporating pharmacy claims data into electronic medication reconciliation. Am J Health Syst Pharm. 2015;72:212-217. [go to PubMed]
25. Carter JA, Carr LS, Collins J, et al. STAAR: improving the reliability of care coordination and reducing hospital readmissions in an academic medical centre. BMJ Innov. 2015;1:75-80. [go to PubMed]
26. Phatak A, Prusi R, Ward B, et al. Impact of pharmacist involvement in the transitional care of high-risk patients through medication reconciliation, medication education, and postdischarge call-backs (IPITCH Study). J Hosp Med. 2016;11:39-44. [go to PubMed]
27. Rosen S, Bailey D, Kamiya E, et al. Geriatric pharmacy pilot's effect on reducing 30-day readmission rates on a geriatric special care unit. Am J Med Qual. 2014;(suppl 30).
28. McGalliard B, Rosen S, Shane R. Safe medication transitions in frail patients. Presented at: ASHP 2015 Midyear Clinical Meeting; December 6–10, 2015; New Orleans, LA.
29. Husebø AML, Storm M. Virtual visits in home health care for older adults. Sci World J. 2014:1-11. [Available at]
30. Moultry AM, Pounds K, Poon IO. Managing medication adherence in elderly hypertensive patients through pharmacist home visits. Consult Pharm. 2015;30:710-719. [go to PubMed]
31. Shane R, Abramowitz PW. Choosing Wisely: pharmacy's role in effective use of medications. Am J Health-Syst Pharm. 2015;72:1529-1530. [go to PubMed]
32. American Geriatrics Society. Ten things clinicians and patients should question. Philadelphia, PA: Choosing Wisely; April 23, 2015. [Available at]
33. Schmader KE, Hanlon JT, Pieper CF, et al. Effects of geriatric evaluation and management on adverse drug reactions and suboptimal prescribing in the frail elderly. Am J Med. 2004;116:394-401. [go to PubMed]
34. Fenton JJ, Levine MD, Mahoney LD, Heagerty PJ, Wagner EH. Bringing geriatricians to the front lines: evaluation of a quality improvement intervention in primary care. J Am Board Fam Med. 2006;19:331-339. [go to PubMed]
35. Kojima G, Bell C, Tamura B, et al. Reducing cost by reducing polypharmacy: the polypharmacy outcomes project. J Am Med Dir Assoc. 2012;13:818.e11-818.e15. [go to PubMed]
36. Tamura BK, Bell CL, Lubimir K, Iwasaki WN, Ziegler LA, Masaki KH. Physician intervention for medication reduction in a nursing home: the polypharmacy outcomes project. J Am Med Dir Assoc. 2011;12:326-330. [go to PubMed]
37. Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med. 2010;170:1648-1654. [go to PubMed]
38. Ware GJ, Holford NH, Davison JG, Harris RG. Unit dose calendar packaging and elderly patient compliance. N Z Med J. 1991;104:495-497. [go to PubMed]
Table
Table. Screening Tool for the Development of Adverse Drug Events in Older Patients.| Major risk factors for adverse drug events in geriatric patients | |
|---|---|
| Screening Question | Response |
| Is the patient under the care of multiple physicians? | Yes/No |
| Does the patient have cognitive impairment? | Yes/No |
| Is the patient on more than 5 medications? | Yes/No |
| Is the patient on medications listed on either the Beers or STOPP lists? | Yes/No |
| Does the patient lack family or caregiver support? | Yes/No |
| Does the patient use multiple pharmacies? | Yes/No |
| Is the patient frail? | Yes/No |
| Does the patient have renal insufficiency? | Yes/No |
| Is a language other than English the patient's primary language? | Yes/No |
| Does the patient have a history of medication noncompliance? | Yes/No |
| Does the patient have low health literacy? | Yes/No |
| Does the patient have a history of falls? | Yes/No |
| Has the patient been prescribed an anticoagulant? | Yes/No |
| A "yes" response to any of the above questions indicates the patient may be at increased risk of experiencing adverse drug events | |
Figure
Figure. GERIATRIC Method.