Prolonged DKA in Pregnancy: A Case of Communication Breakdown.
Marshall S, Boe NM. Prolonged DKA in Pregnancy: A Case of Communication Breakdown.. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2023.
Marshall S, Boe NM. Prolonged DKA in Pregnancy: A Case of Communication Breakdown.. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2023.
Patrick Romano, MD, MPH; Debra Bakerjian, PhD, APRN, RN; Amy Nichols, EdD, RN; Nina M. Boe, MD; Sarah Marshall, MD, for this Spotlight Case and Commentary have disclosed no relevant financial relationships with ineligible companies related to this CME activity.
Learning Objectives
- Articulate how breakdowns in communication amongst providers can lead to medical errors and prolonged hospitalization.
- Describe factors contributing to diabetic ketoacidosis (DKA) in pregnancy.
- Identify medications used to safely treat nausea and vomiting in pregnancy.
- Apply principles of team-based care and communication in a culture of safety to improve care in complex health care situations.
The Case
A 31-year-old nulliparous woman with a history of type 1 diabetes, managed successfully with an insulin pump, presented to the Emergency Department (ED) at a gestational age of 6 weeks with 3 days with nausea and vomiting. On arrival, her laboratory tests revealed an elevated white blood cell count of 14,640, high serum glucose values of 157 to 194 mg/dL, a blood urea nitrogen (BUN) to creatinine ratio of 15 (suggesting mild volume depletion), an elevated anion gap of 16, and a beta-hydroxybutyrate level of 17. Maternal Fetal Medicine (MFM), endocrinology, and gastroenterology were consulted.
The patient was admitted to the inpatient internal medicine unit with a diagnosis of diabetic ketoacidosis (DKA). She was given intravenous fluids and continued insulin pump management of her blood glucose. To reduce nausea and vomiting, the primary team initially ordered intramuscular (IM) trimethobenzamide, later substituted ondansetron, and then reached out to the MFM consultant for advice on antiemetic use in pregnancy. The MFM team provided written recommendations and rounded on the patient daily. However, the patient’s symptoms persisted, and she developed a progressively worsening metabolic acidosis with an anion gap peaking at 20.
Several days after admission, while the MFM team was rounding, the patient reported that she was being transferred to another hospital. Subsequently the MFM team reached out to the primary team and recommended transfer to the in-house obstetric service. The patient’s care was assumed by the obstetrics team, and within 12 hours her anion gap was closed. Her nausea and vomiting resolved, and she was discharged home the next day.
The Commentary
By Sarah Marshall, MD, and Nina M. Boe, MD
This case describes a 31-year-old pregnant patient with type 1 diabetes on an insulin pump who was hospitalized for euglycemic diabetic ketoacidosis (DKA). She was treated for dehydration and vomiting, but not aggressively enough, and her metabolic acidosis worsened over several days. The primary team hesitated to prescribe medications despite their safety in pregnancy and delayed reaching out to the MFM consultant. The consultant made recommendations but did not ensure that the primary team received and understood the information. Presumably there was no direct communication between these providers until several days after admission, triggered by an impending transfer to an outside hospital. When that communication finally happened, it improved the patient’s course of care. Instead of being transferred to an outside hospital, the patient was transferred to a different service, her DKA resolved rapidly, and she was discharged. The physicians in this case were not communicating effectively, nor were they functioning as a team, which put patient safety at risk and resulted in a prolonged hospitalization.
Approach to Improving Safety & Patient Safety Targets
Euglycemic DKA in pregnant patients
DKA is an acute, potentially life-threatening complication of diabetes mellitus (DM). Euglycemic DKA is defined as ketoacidosis in the absence of pronounced hyperglycemia and affects up to 5% of all diabetic pregnancies.1,2 While more common with type 1 DM, euglycemic DKA can also occur in patients with type 2 DM. In pregnancy, it can occur in patients with either pregestational or gestational diabetes. A 2020 study in the United Kingdom reported an incidence of DKA of 6.3 per 100,000 pregnancies. Half of the episodes of DKA were euglycemic, and approximately 15% of patients with DKA had more than one episode during pregnancy.3 Identifying DKA in pregnancy is challenging because the presentation is often vague, and onset can be rapid. Nausea and vomiting are often prominent presenting features of DKA, but these symptoms are also common during normal pregnancies. Precipitating factors for DKA include infections, new-onset diabetes, insulin pump failure or missed doses, hyperglycemia-inducing medications such as oral steroids, and diabetic gastroparesis (leading to erratic oral intake and delayed gastric emptying).
Managing euglycemic DKA requires aggressive volume replacement with intravenous fluid, correction of electrolyte abnormalities, and intravenous insulin therapy. These authors recommend providers follow the American College of Obstetricians and Gynecologists’ (ACOG) guidelines for managing DKA in pregnancy.4,5 For patients who use an insulin pump (as the patient in this case did), providers should have heightened awareness of the risk of pump malfunction, most commonly due to kinking, blocking, or dislodgement of the infusion catheter.6 Patients treated with continuous subcutaneous insulin infusions may have a higher rate of DKA episodes than patients receiving multiple daily injections (e.g., 13% compared with 1.6%, P=.04, in one study7), although systematic reviews have not shown convincing evidence to support the use of one form of insulin administration over another for pregnant women with diabetes.8
Safe Medication Prescribing in Pregnancy-Associated Nausea and Vomiting
Choice of medications in pregnancy should include considerations of overall efficacy, safety, and gestational age. Many resources exist to aid providers including an algorithm developed by ACOG for managing nausea and vomiting in pregnancy.9,10 It outlines a range of non-pharmacologic options as first line, including eating small frequent meals, avoiding spicy or fatty foods, eliminating supplemental iron, and avoiding sensory stimuli (e.g., odors, heat) that may provoke nausea. Ginger capsules (250 mg four times daily) may reduce nausea but have no apparent benefit in reducing vomiting. If symptoms persist, the guideline recommends adding vitamin B6 (pyridoxine) 10-25 mg orally (either alone or in combination with doxylamine 12.5 mg), three or four times daily. A systematic review of randomized controlled trials (RCTs) found a paucity of high-quality evidence,11 but a recent systematic review of both RCTs and non-RCTs found that pyridoxine was associated with improvement in mild nausea and vomiting.12
Antihistamines or phenothiazines, such as dimenhydrinate, diphenhydramine, prochlorperazine or promethazine are recommended next. All of these medications are given orally except for prochlorperazine and promethazine, which can also be given rectally. At this point in the algorithm, providers must evaluate hydration status. If the patient is not dehydrated, the guideline recommends adding metoclopramide (oral or IM), ondansetron (oral), promethazine (oral, rectal, or IM), or trimethobenzamide (IM). However, for dehydrated patients, intravenous fluid replacement and medications are recommended (i.e., dimenhydrinate, metoclopramide, ondansetron, or promethazine).
In this case, the primary team initially chose trimethobenzamide, a dopamine receptor antagonist, and then switched to ondansetron, a serotonin 5-hydroxytryptamine (type 3) receptor antagonist, to manage the patient’s vomiting. It is possible that they used the algorithm but incorrectly assessed that the patient was not dehydrated. A more likely scenario is that they chose familiar medications, considering safety in pregnancy as an afterthought. Trimethobenzamide and ondansetron have limited evidence of safety in pregnancy. When taken at higher doses, ondansetron can prolong the QT interval and may increase the chance of cleft palate when used in the first trimester.13,14 Had the primary team clearly and directly communicated their questions about medication use in pregnancy to the consultant, or if the MFM consultant had ensured that the primary team received and understood their medication recommendations, it would have improved the patient’s care.
Systems Change Needed / Quality Improvement Approach
In complex health care situations, such as our case of a patient who was in her first trimester of pregnancy and developed DKA, good communication and teamwork are critical. When communication breaks down, patient safety can be compromised. More than twenty years after Institute of Medicine’s (IOM) landmark report “To Err is Human,” we are still struggling to improve safety in healthcare. Optimizing patient safety culture and building better teams are listed as two of the ten “Patient Safety Tips for Hospitals” recommended by the Agency for Healthcare Research and Quality (AHRQ). A recent cross-sectional study of patient safety culture and teamwork in intrapartum care demonstrated that healthcare professionals’ perceptions of patient safety culture and teamwork were significant for overall patient safety.15
Communication in a Culture of Safety
Creating a culture of safety builds shared values and norms amongst interprofessional teams. These values and norms then serve to guide teams’ behaviors. While there are many aspects to creating a culture of safety, communication is a key component. When communication breaks down, patient safety can be compromised, often leading to inefficient use of valuable resources. Key behaviors to emphasize in a patient safety culture include the following:
- Encourage questions (for clarification or to increase knowledge).
- Communicate directly (ideally face to face or at least talking together).
- Conduct shared (or team-based) patient rounds and discussions of management plans.
- Create a blame-free environment in which individuals can report errors or near misses without fear of reprimand or punishment.
- Collaborate across ranks and disciplines to seek solutions to patient safety problems.
- Provide patient safety culture training to all providers.
- Use shared language. Several tools can help:
- SBAR (Situation, Background, Assessment, Recommendation).
- CUS Words (“I am Concerned,” “I am Uncomfortable,” “This is a Safety Issue”).
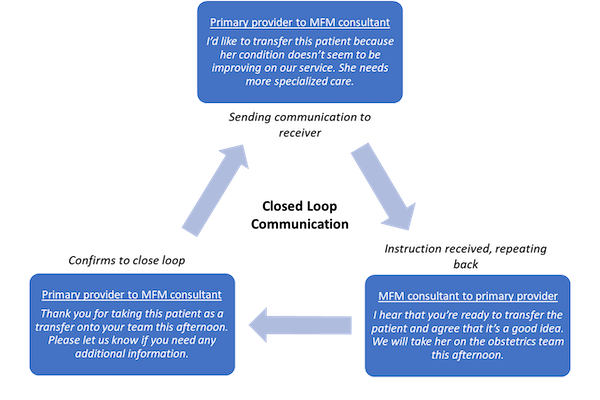
- Closed Loop Communication: sender gives an instruction to a receiver, the instruction is received, the receiver repeats it back, the sender confirms to close the loop.
Team-Based Care
The complexity of our constantly evolving health care system necessitates that care delivery occurs in a team-based structure. Health care teams are multidisciplinary, bringing together professionals from different fields to determine and deliver patients’ treatment. When pregnant patients are hospitalized with acute medical illnesses, primary providers can include midwives, obstetricians, family medicine physicians or internists, and multiple specialist physicians may be part of the team. The specific primary and specialty team composition depends on the hospital’s volume and resources. Given this variability, it is critical that teams have shared norms. The National Academy of Medicine’s discussion paper on team-based health care offers principles that can guide health care teams in a variety of settings:16
- Shared goals: Establish shared goals that reflect patient and family priorities and can be clearly articulated, understood, and supported by all team members.
- Clear expectations: Set clear expectations for each team member’s functions and responsibilities to optimize efficiency. The team can accomplish more than the sum of its parts.
- Mutual trust: Team members earn each other’s trust, creating norms of reciprocity and greater opportunities for shared achievement.
- Effective communication: The team prioritizes and continuously refines its communication skills. Consistent channels are accessed and used by all team members across settings.
- Measurable processes and outcomes: The team agrees on and implements reliable and timely feedback on successes and failures. These are used to track and improve performance.
Had the health care providers in our case utilized these principles, the patient’s DKA might have been treated in a more timely and effective manner. Let us demonstrate how this case might have gone differently if the providers had used appropriate tools in their communication with each other.
Example of SBAR (Primary provider to MFM consultant):
- Situation: I am caring for a patient who is vomiting with a BUN-to-creatinine ration of 15
- Background: She is 6 weeks pregnant and in DKA
- Assessment: Oral therapy has not been sufficient
- Recommendation: I think she needs medications that are safe during pregnancy. What do you recommend?
Example with CUS Words (MFM consultant to primary provider):
- C: I’m concerned that she’s still dehydrated.
- U: I’m uncomfortable with her anion gap increasing.
- S: This is a patient safety issue.
Example of Closed Loop Communication:
Take-Home Points
- Caring for pregnant patients with acute medical illnesses such as DKA is optimally done by a collaborative, coordinated team.
- Providers should consider safety for the fetus before prescribing medications to pregnant patients. For example, ondansetron is a third-line medication for nausea and vomiting in pregnancy; metoclopramide, antihistamines, and phenothiazines are considered safer choices.
- All health care providers should receive training about patient safety culture and working in interprofessional teams.
- SBAR, CUS words, and Closed Loop communication are tools that health care providers can use to improve communication.
Sarah Marshall, MD
Health Sciences Clinical Professor
Department of Family and Community Medicine
UC Davis Health
smarshall@ucdavis.edu
Nina M. Boe, MD
Professor
Department of Obstetrics and Gynecology
UC Davis Health
nmboe@ucdavis.edu
References
- Nasa P, Chaudhary S, Shrivastava PK, et al. Euglycemic diabetic ketoacidosis: a missed diagnosis. World J Diabetes. 2021;12(5):514-523. [Free full text]
- Gomez-Rios MA, Gomez-Rios D, Paech MJ, et al. Managing diabetic ketoacidosis in pregnancy. Saudi J Anaesth. 2016;10(2):238-9 [Free full text]
- Diguisto C, Strachan MWJ, Churchill D, et al. A study of diabetic ketoacidosis in the pregnant population in the United Kingdom: investigating the incidence, aetiology, management and outcomes. Diabet Med. 2022 Apr;39(4):e14743. [Free full text]
- ACOG Practice Bulletin No. 201: Pregestational Diabetes Mellitus. Obstet Gynecol. 2018;132(6):p e228-e248. [Available at]
- Sibai BM, Viteri OA. Diabetic ketoacidosis in pregnancy. Obstet Gynecol. 2014 Jan;123(1):167-178. [Available at]
- Crabtree TSJ, Gazis A. Insulin pumps and diabetes technologies in pregnancy: an overview for the obstetrician. Obstetrics, Gynaecology & Reproductive Medicine. 2020;30(4):126-129. [Free full text]
- Chen R, Ben-Haroush A, Weismann-Brenner A, et al. Level of glycemic control and pregnancy outcome in type 1 diabetes: a comparison between multiple daily insulin injections and continuous subcutaneous insulin infusions. Am J Obstet Gynecol. 2007;197(4):404.e1-5. [Available at]
- Farrar D, Tuffnell DJ, West J, et al. Continuous subcutaneous insulin infusion versus multiple daily injections of insulin for pregnant women with diabetes. Cochrane Database Syst Rev. 2016;2016(6):CD005542. [Free full text]
- Medications and Pregnancy. National Institutes of Health Office of Research on Women’s Health. Accessed June 26, 2023. [Available at]
- ACOG Practice Bulletin No. 189: Nausea and Vomiting Of Pregnancy. Obstet Gynecol. 2018;131(1):e15-e30. [Available at]
- Matthews A, Haas DM, O’Mathúna DP, et al. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2015;(9):CD007575. [Free full text]
- McParlin C, O’Donnell A, Robson SC, et al. Treatments for hyperemesis gravidarum and nausea and vomiting in pregnancy: a systematic review. JAMA. 2016;316(13):1392–401. [Available at]
- Mother To Baby | Fact Sheets [Internet]. Brentwood (TN): Organization of Teratology Information Specialists (OTIS); 1994-. Ondansetron (Zofran®) 2022 Sep. [Available at]
- Hansen WF, Peacock AE, Yankowitz J. Safe prescribing practices in pregnancy and lactation. J Midwifery Womens Health. 2002;47(6):409-21. [Free full text]
- Skoogh A, Bååth C, Hall-Lord ML. Healthcare professionals' perceptions of patient safety culture and teamwork in intrapartum care: a cross-sectional study. BMC Health Serv Res. 2022;22(1):820. [Free full text]
- Mitchell P, Wynia M, Golden R, et al. Core principles & values of effective team-based health care. NAM Perspectives. Washington, DC: National Academy of Medicine; 2012. [Free full text]