The Fluidity of Diagnostic "Wet Reads"
Lee CS, Hess CP. The Fluidity of Diagnostic "Wet Reads". PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2016.
Lee CS, Hess CP. The Fluidity of Diagnostic "Wet Reads". PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2016.
The Case
A 64-year-old man with heavy tobacco use presented to the emergency department (ED) with chest pain. His electrocardiogram showed no evidence of myocardial ischemia, but his blood pressure was markedly elevated. The treating physician, concerned about a possible aortic dissection, ordered a CT angiogram of the chest. The preliminary ("wet") read from the radiologist was communicated to the ED physician—it reported "no evidence of aortic dissection," so the patient was discharged home once his symptoms resolved. He was advised to establish care with a primary care physician (PCP). A final read of the CT scan would be performed the following morning, but by then the patient was already home and no clinician reviewed it that day.
The patient saw his new PCP about 1 month later and reported fatigue, a chronic nonproductive cough, and a 17-pound weight loss over the past year. He brought his printed after-visit summary (AVS) from the ED visit, which noted that a chest CT had been performed, which showed no aortic dissection. After reviewing the AVS, the PCP assumed there were no other concerning findings on the CT scan. As it was a very busy clinic day, he did not review the final radiology report for the CT scan. The PCP counseled the patient on tobacco cessation and obtained basic lab tests to work up his fatigue and weight loss. He scheduled the patient for a follow-up visit in 1 month.
The patient missed this follow-up appointment and ultimately returned to the clinic several months later. At that point, he told the PCP that his cough had worsened and was now producing blood-tinged sputum. Concerned, the PCP immediately obtained a chest radiograph, which showed a large right upper lobe nodule. Only then did the PCP review the formal report from the earlier CT—which had documented "a suspicious noncalcified, spiculated nodule in the right upper lobe of the lung measuring approximately 1.2 cm in diameter, concerning for malignancy given the patient's history of tobacco use"—and realize that the nodule had been seen previously. It was not clear if any physician had been informed about the lung nodule after the final reading of the earlier CT was issued. The patient was ultimately diagnosed with primary lung adenocarcinoma involving the right upper lung.
The error was disclosed to the patient with the help of clinic leadership and risk management. The patient was understandably upset that he was not made aware of the initial findings, but he continued working with providers to expedite his care.
The Commentary
by Cindy S. Lee, MD, and Christopher P. Hess, MD, PhD
Evolution of Wet Reads
The case outlined above highlights the inherent risks of communication breakdown between services within our current medical system. In most hospitals across the United States, radiographs performed during off hours are interpreted twice. The concept of an initial "wet" interpretation has evolved over time as technology for image review has changed. Before the digital era, films were developed in solutions followed by a lengthy drying process. Radiologists reviewing the wet printed film issued a "wet read." Nowadays, the films have been replaced by digital images, but we still refer to the preliminary readings by trainees or "nighthawk" radiologists as wet reads. Their purpose is to permit timely identification of abnormalities that mandate emergent treatment. The following morning, an attending or staff radiologist issues the final, formal report that summarizes all relevant, actionable findings. No longer constrained by printed film, thousands of images from a single study are now available for review in near real time. In the past, detailed conversation between services to share patient history and discuss study results often took place in radiology reading rooms. The electronic medical record now serves as the primary vehicle for communicating the history and physical examination, and faxed or electronic wet reads serve as the new instrument to convey the results of imaging.
Frequency and Significance
The frequency and significance of the discrepancies between preliminary and final interpretations have been evaluated in multiple studies. At our institution, wet reads are documented in the electronic medical record, then tracked and adjudicated by division quality champions. In 2015, 0.29% of CT wet reads were noted to have a major discrepancy, defined as a misinterpretation in the wet read that would significantly alter short-term treatment, at final review. This compares favorably with national benchmarks of 1%–2.3% for major discrepancy.(1-3) This wet read system has evolved over the years; it now prioritizes wet reads containing emergent findings so that these studies are reviewed first by attending radiologists the following morning and acted upon earlier if discrepancy is found.(3)
Subcritical Findings: System Solution
Clear guidelines and policies are in place for communication of critical findings.(2) In contrast, subcritical findings—nonemergent findings that require follow-up but do not pose an immediate threat—open the door for communication error. This case emphasizes the potential impact of subcritical findings on long-term patient outcomes, as some incidental lung nodules may harbor malignancy. Subcritical findings were found in approximately 3.3% of cases at our institution in 2015, comparable to 3%–7% in the literature.(3)
It is incumbent upon health care systems to develop better approaches to ensure adequate communication between providers. To bridge this care gap, we implemented an innovative system-wide solution—the UCSF Relay Center—in 2011 to facilitate reporting of subcritical findings to providers. Subcritical findings requiring short-term follow-up, such as incidental lung nodules, are marked with key words in radiology reports and culled electronically for communication to providers. Flagged reports are processed by administrative staff, who contact both ordering and primary providers to relay text within reports that has been annotated as subcritical. In the future, there is ongoing discussion as to whether patients should be alerted directly when additional evaluation is necessary after imaging. The full text of reports is also made available to patients through an electronic medical information portal after a 5-day embargo, a period allotted to permit providers to contact patients with results. The threshold for follow-up or future management for subcritical findings is determined by their risk for adverse patient outcome.
Incidental Pulmonary Nodules
Pulmonary nodules are a common incidental finding in up to 31% of chest CTs performed for other reasons (4) and in 15%–50% of patients undergoing CT lung cancer screening.(5,6) The rise in CT use for both diagnosis and lung cancer screening means that more incidental nodules will be detected in the future.
Follow-up and Management of Pulmonary Nodules
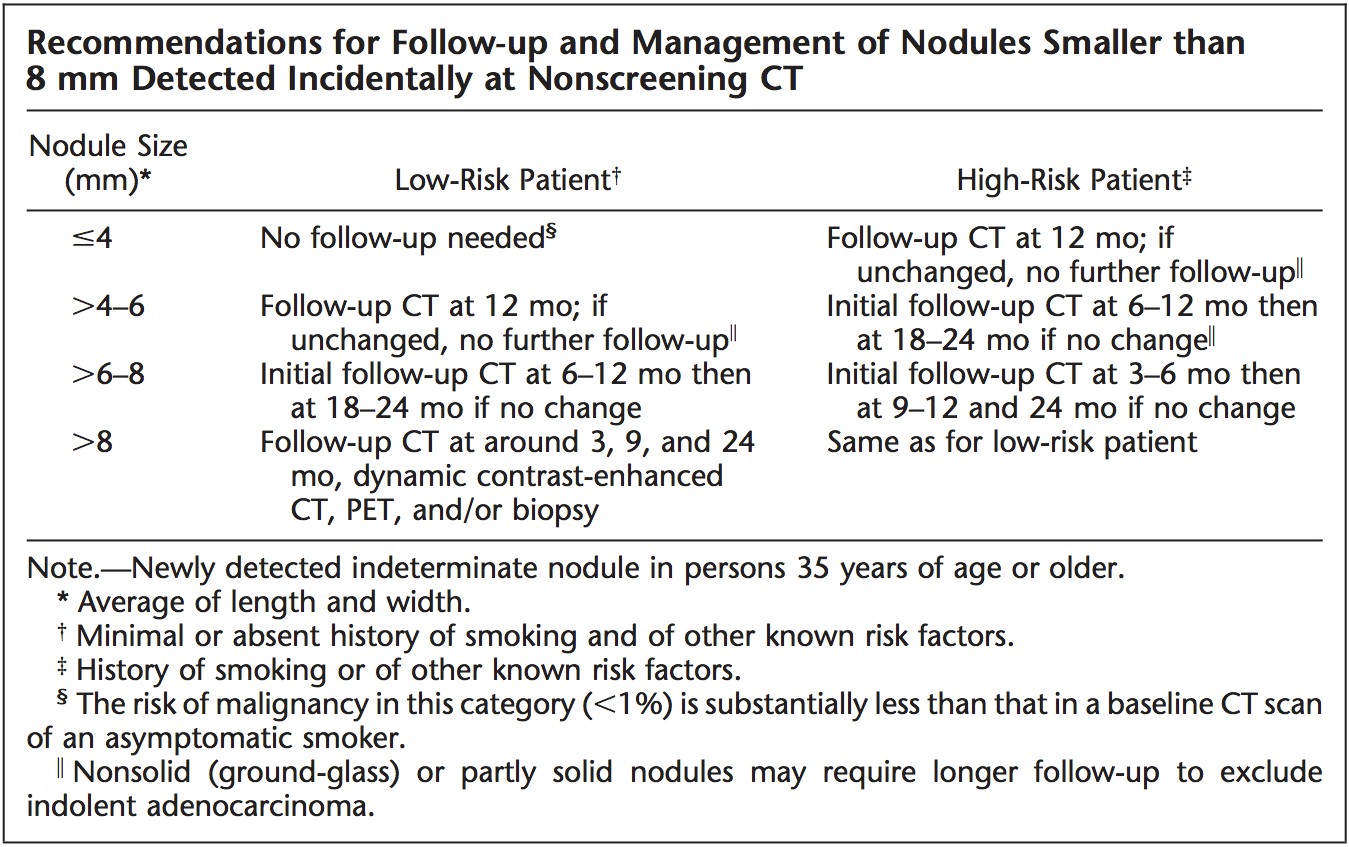
Suspicious-appearing nodules (such as those with larger size, spiculated border, rapid growth, and high density) require immediate work-up to exclude malignancy. Alternatively, nodules with any of the three findings of (i) benign pattern of calcification; (ii) gross fat; or (iii) long-term stability (≥ 2 years for solid nodules) require no follow-up. CT surveillance is recommended for nodules with indeterminate CT appearance and low risk of malignancy. The most widely cited recommendation, the 2005 Fleischner Society guidelines, stratified the surveillance protocol based on the nodule size and patient risk profile.(7) These guidelines are shown in the Table and are in agreement with the American College of Chest Physicians (ACCP) recommendations.(4)
Despite widespread acceptance of these guidelines, important new evidence regarding subsolid nodules have come to light. These are summarized in the updated 2013 Fleischner and ACCP guidelines. Although subsolid nodules are often malignant or premalignant, they usually give rise to malignancies that behave more indolently than those arising from solid nodules. For this reason, subsolid nodules may require extended CT surveillance for growth or development of their solid component. A second key distinction in the 2013 Fleischner guidelines is that patients with history of smoking are no longer differentiated from ex-smokers or nonsmokers, partly due to rising incidence of adenocarcinoma in younger and nonsmoking individuals.(8) This case is a reminder of the need for such a systematic approach to the management of incidental pulmonary nodules.
Addressing incidental and discrepant findings in a consistent manner is possible by adopting a systematic solution that alerts the referring physicians about clinically actionable findings. The Relay System we have developed demonstrates that a department-wide approach to communicating subcritical imaging findings can be implemented with minimal physician burden. If such a system had been in place at the radiology department where this patient's initial imaging was performed, the delay in diagnosis of lung cancer could have been prevented. Given the increasing recognition of systems issues as a major contributor to diagnostic errors, radiology departments should take steps to establish formal systems for communicating both critical and subcritical imaging findings to referring physicians.
Take-Home Points
- The rates of major discrepancy between preliminary ("wet") reads of radiology studies and final review—defined as a misinterpretation in the wet read that would significantly alter short-term treatment—range from 1%–2.3% in the literature, although some systems are able to do better.
- Pulmonary nodules are common incidental findings on up to 31% of chest CTs. No follow-up is necessary if one of the three benign CT features is present: (i) benign pattern of calcification; (ii) gross fat; or (iii) long-term stability (≥ 2 years for solid nodules).
- Suspicious CT features of pulmonary nodules include larger size, spiculated border, growth, and density. Suspicious-appearing nodules require immediate work-up to exclude malignancy. CT surveillance is recommended for nodules with indeterminate CT appearance and low risk of malignancy.
- Although subsolid nodules are more often malignant or premalignant, they usually give rise to malignancies that behave more indolently than solid malignancies. For this reason, subsolid nodules may require extended CT surveillance for growth or development of solid component.
- Radiology departments should develop robust systems to track their wet read error rates and to inform frontline clinicians when a major discrepancy is found during the final reading.
Cindy S. Lee, MD Department of Radiology and Biomedical Imaging University of California, San Francisco San Francisco, CA
Christopher P. Hess, MD, PhD Department of Radiology and Biomedical Imaging University of California, San Francisco San Francisco, CA
References
1. Issa G, Taslakian B, Itani M, et al. The discrepancy rate between preliminary and official reports of emergency radiology studies: a performance indicator and quality improvement method. Acta Radiol. 2015;56:598-604. [go to PubMed]
2. Ruutiainen AT, Scanlon MH, Itri JN. Identifying benchmarks for discrepancy rates in preliminary interpretations provided by radiology trainees at an academic institution. J Am Coll Radiol. 2011;8:644-648. [go to PubMed]
3. Arenson R. The wet read [Spotlight]. AHRQ WebM&M [serial online]. March 2006. [Available at]
4. Gould MK, Tang T, Liu IL, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med. 2015;192:1208-1214. [go to PubMed]
5. Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience. Radiology. 2005;235:259-265. [go to PubMed]
6. Henschke CI; International Early Lung Cancer Action Program Investigators. Survival of patients with clinical stage I lung cancer diagnosed by computed tomography screening for lung cancer. Clin Cancer Res. 2007;13:4949-4950. [go to PubMed]
7. MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005;237:395-400. [go to PubMed]
8. Naidich DP, Bankier AA, MacMahon H, et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society. Radiology. 2013;266:304-317. [go to PubMed]
Figure
Figure. Short-term Follow-up of Ground-Glass Nodule on CT: (a) baseline; (b) 6 months.Consecutive CT images through left lower lobe obtained at same anatomic level after 6 months show rapid transformation of initial pure ground-glass nodule (a) to a mixed solid–ground-glass nodule (b), which subsequently proved to be mucinous adenocarcinoma.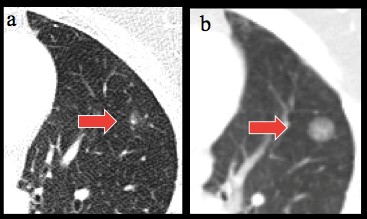
Table
Table. Fleischner Society Recommendations for Solid Pulmonary Nodules. Reprinted with permission from (7) MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005;237:395-400.