Medication Reconciliation Pitfalls
The Case
A 90-year-old woman who lived alone suffered a mechanical fall with subsequent hip fracture and was brought to the emergency department (ED) by her daughter. The patient had a past medical history of hypothyroidism, osteoarthritis, and hypertension. The patient's medication bottles were given to the ED triage nurse and were used to generate a list of home medications. Among others, the list included "Toprol-XL 75 mg po daily." An orthopedic surgeon admitted the patient to the hospital and wrote orders to continue all of her home medications at their prior dosages. The surgeon also requested an internal medicine consultation for "preoperative clearance." The patient denied any history of arrhythmia, syncope, presyncope, dementia, or prior falls. Her medications were placed in an opaque, plastic personal-belongings bag along with her clothes, and she was moved to the orthopedic floor.
Several hours later, the consulting hospitalist performed an evaluation and confirmed the patient's home medications and their dosages. Other than her leg trauma and a mild hearing deficit, the patient's examination was normal. She did not inform the hospitalist that the medications were in her hospital bag; in fact, she may not have even realized that her daughter had left them there with her. The hospitalist noted a heart rate of 75 beats per minute with a systolic blood pressure of 170 mmHg. Blood pressure readings had been high since admission. An order was written to increase Toprol-XL from 75 mg to 100 mg daily.
While being prepped on the operating room table several hours later, the patient developed asystole, underwent successful resuscitation, and was transferred to the ICU. Upon transfer, an ICU nurse handed the plastic bag of medications to the consulting cardiologist who noted that the patient's home dosage of Toprol-XL was 25 mg daily. The error was reported to the hospital pharmacy. Only by coincidence did the hospitalist who had increased the Toprol-XL dosage learn of the error. The hospitalist apologized to the patient and her family and assured them that the case would be carefully reviewed to ensure that a similar error wouldn't happen again.
The patient made a full recovery and had no recurrent vital sign instability. Myocardial infarction was ruled out, and an echocardiogram was normal. After observation in the ICU for several days, she underwent repair of her hip fracture and was discharged to home without further complications.
The Commentary
This error involves a system failure in the proper identification, documentation, and storage of a patient's medications brought from home. The admission dosage of metoprolol extended-release (Toprol-XL®) was incorrectly transcribed from the patient's prescription bottle. To further aggravate the problem, the errant metoprolol dose was increased in response to this elderly patient's persistent tachycardia and systolic hypertension, resulting in a fourfold metoprolol overdose. This overdose was the apparent cause of a catastrophic cardiac arrhythmia (called "asystole" in the case report but more likely complete heart block). Fortunately, the patient survived with no lasting effects.
Problem Description
Errors in the drug name, dosage, frequency, and route of administration for home medications continued on hospital admission are common. In fact, these errors and their serious consequences prompted requirements in hospitals for medication reconciliation as a critical safety program.(1) MEDMARX™ (Quantros, Inc.; Milpitas, CA), a web-based national medication error reporting system, received 2567 error reports involving medication reconciliation during 2008-2009. Of these errors, 45 events involved the patient's home medication.(2) These events included omitted dosages on admission, incorrect drug prescribed/administered, and improper dosage or frequency compared with patients' home medication regimens. Other common anecdotes related to misadventures regarding patients' home medications include lost or stolen medications (particularly expensive drugs, antibiotics, steroids, or narcotics), as well as damaged and contaminated medication.
Root Causes
Causes of errors involving patients' home medications include (i) failing to bring the medication bottles to the hospital and relying on a medication list, (ii) limited or no access to vital patient information needed to correctly prescribe home medications on admission, (iii) unclear packaging/labeling of home medications, and (iv) staff with limited experience in evaluating home medications. Importantly, serious errors (harm) related to patients' home medications as reported by MEDMARX™ occurred exclusively during the admission process.
Process Variation
The health care professionals in this case failed to accurately review and document the patient's prescription bottles from home. The error was initiated and perpetuated after the ED triage nurse incorrectly transcribed the metoprolol dosage as 75 mg XL; furthermore, the home medications were misplaced. Additionally, the error was propagated by the surgeon, who incorrectly copied the medication list from the ED triage nurse on the admission orders. Finally, the hospitalist adjusted therapy based on an incorrect dose, causing the adverse drug event.
Solutions
Properly identify home medications.
In this case, the preoperative assessment should have included a review of home medication bottles along with a verification of those medications against the patient's medication list. For elective admissions, the preoperative outpatient visit is an ideal setting for conducting a patient medication history, and allows for adequate time to inspect the patient's prescription bottles from home and complete a medication list. However, since this patient was admitted emergently, an outpatient preoperative assessment was not feasible. In such a case, having the patient's home medications verified by a hospital pharmacist may have prevented the error. Hospitals with pharmacy staffing on the nursing units can incorporate this function in the pharmacy admission assessment. In hospitals without this pharmacist staffing, developing a collaborative approach using nurses or pharmacy technicians focusing on high-risk patients (e.g., elderly patients; patients with more than 10 medications at home) will mitigate mix-ups. Allowing for at least two health care professionals in verifying the identity, dosage, and instructions for home medications provides a safe, manual system for documenting patients' home medications.
This case emphasizes the importance of including pharmacists in review of home medication. A pharmacist's familiarity with available dosage forms may have prevented this error, since metoprolol XL is not available as a 75-mg dosage—only 25-mg and 50-mg tablets. Also, many medications available as generic formulations physically look quite different from the corresponding trade-name products; in such cases, expert review can facilitate proper identification. Furthermore, patients often place several medications into the same container, making it difficult to accurately identify home medications. As a result, involving the pharmacist as a resource or using Web-based subscription resources for tablet/capsule identification (e.g., www.drugid.info) can help to properly identify medications. A recently published report showed that medication identification services can be effectively provided by certified poison centers using automated, interactive voice recognition software.(3)
Effectively communicate home medication reconciliation.
In this case, the hospitalist was unaware of the error in metoprolol dosage. A progress note documented in an electronic medical record that is viewed across all patient encounters may have provided valuable information to this physician when assessing the effect of the patient's beta-blocker therapy.
Use technology for handling and storage of home medications.
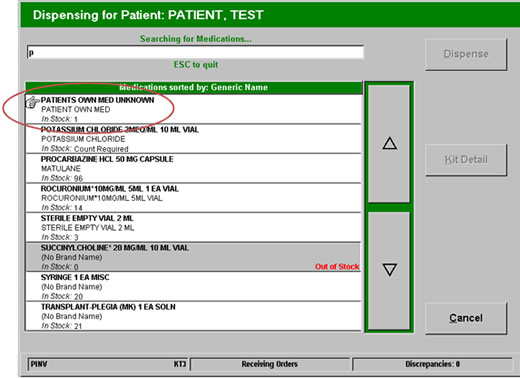
A recent Australian study showed that patients who physically brought their medication into the hospital had fewer admission prescribing errors compared to those who did not.(4) However, medication bottles must be appropriately handled. Applying systematic and standardized "chain of custody" procedures for this patient's home medication may have prevented this error by making the medications available for inspection (Figure 1). Electronic documentation of handling of home medications can be customized in most automated dispensing devices to store patients' home medications (Figure 2). Except in emergency situations, computer entry systems may be adapted to provide a "hard stop" on admission medication orders written based on home medication bottles until they are inspected and reviewed by a pharmacist.
Handling patients' home medication requires a systematic method to prevent prescribing errors. Doing it right often requires diligence and attention to detail as well as cooperation from patients. By combining technology solutions—standardized approaches to review, documentation, and handling of patients' own medications—and a focus on direct communication among caregivers and patients, the incidence and severity of errors involving patients' home medications can be reduced.
Patients may be allowed to take their medications from home while in the hospital—this is mainly done in instances when the medication is hard to obtain (e.g., Revlimid [lenalidomide], a specialty oral medication for multiple myeloma) or in case of financial hardship. These cases may be justified to avoid any delay or problem with therapy—provided that all of the safeguards for ensuring product integrity are followed. More importantly, writing vague orders such as "medications as at home" can be confusing and leave too many things up to interpretation by physicians and others, resulting in missed, or even wrong, medications being ordered for admission.
Take-Home Points
This medication error illustrates several key points about enhancing the safety of handling patients' medications from home:
- Develop a process for systematic review and disposition of medications from home during the admission process or preadmission visit. At least two persons should inspect and verify the actual prescription bottles for dosage and directions.
- Medications that cannot be sent home with the patient's family or guardian should be secured using available pharmacy automation.
- An electronic progress note that verifies the patient's medications from home should be written by a health care professional and made available across all patient encounters.
- Prohibit orders such as "medications as at home," to avoid confusion in verifying the patient's home medications
Robert J. Weber, PharmD, MS
Associate Professor and Chair
University of Pittsburgh School of Pharmacy
Executive Director of Pharmacy
University of Pittsburgh Medical Center
References
1. Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205. [go to PubMed]
2. MEDMARX™ data search. [Available at]
3. Krenzelok EP, Mrvos R. The use of an automated interactive voice response system to manage medication identification calls to a poison center. Clin Toxicol. 2009;47:425-429. [Available at]
4. Chan EW, Taylor SE, Marriott JL, Barger B. Bringing patients' own medications into an emergency department by ambulance: effect on prescribing accuracy when these patients are admitted to hospital. Med J Aust. 2009;191:374-377. [go to PubMed]
Figures
Figure 1. Process flow for patients' own medications.
Figure 2. Screen shot of automated dispensing device for storing patients' own medication.