Workaround Error
The Case
A retired 81-year-old physician with metastatic colon cancer was admitted to an acute care hospital with pneumonia and congestive heart failure (CHF). After his acute hospitalization, he was transferred to a skilled nursing unit to complete antibiotic therapy. Cancer chemotherapy was scheduled to begin after discharge.
Three days after transfer to the skilled nursing unit, the patient complained of nausea. Intravenous ondansetron (Zofran) was ordered. Approximately 1 hour after the first dose of ondansetron, he was found unresponsive and in respiratory distress. Stat labs were ordered, and his blood glucose was 23 mg/dL. The patient had no history of diabetes or hypoglycemia.
He was given glucagon and transferred to the intensive care unit. Laboratory studies showed an insulin level of greater than 1500 micro-units/mL (upper end of the reference range: 17 micro-units/mL). Intravenous glucose and glucagon were continued, and his blood glucose stayed in the low 40 mg/dL range for several days. Ultimately, he was discharged without any permanent disability from the event, but he was in a weakened state and his chemotherapy was delayed.
The incident led to an internal review of the case. In this skilled nursing unit, many of the nurses remove medications from the Pyxis machine (an automated dispensing device) and insulin from the refrigerator and place them in portable medication carts that are then taken to the bedside. The nurse who was caring for the patient the night of the first ondansetron dose worked infrequently and had an especially heavy workload that evening (she was caring for nine patients on her shift). When her portable medication cart was inspected, ondansetron and insulin vials were found to be next to each other. It was presumed that she mistakenly administered insulin instead of ondansetron.
The Commentary
Inadequate staffing ratios, hurriedness, distractions, and workarounds can adversely affect outcomes for patients in acute care settings.(1) These causes, and lack of familiarity with the nursing unit, seem to have been contributing factors in this case.
Automated dispensing machines (ADMs) (Figure 1) have replaced the traditional cassette system in many hospitals, because they allow medications to be stored safely and retrieved quickly, and they facilitate tracking of medication charges. Indeed, ADMs have improved medication availability, increased the efficiency of drug dispensing and billing, and increased time for other patient care activities. They have also been proposed to decrease medication errors.(2) However, the use of ADMs may lead to workarounds, just as occur with old-fashioned medication cart systems.
In this case, the safety features of the ADM were bypassed on the nursing unit by the use of the portable medication cart (Figure 2). With ADMs, medications are stored in separate labeled bins, and the machine has an intelligent system or computerized list of each patient’s name and their ordered medications. When the medication is selected on the ADM touch screen, the correct drawer opens. At the same time, the medication name and location are identified on the screen. The nurse then selects the correct drug from the drawer.
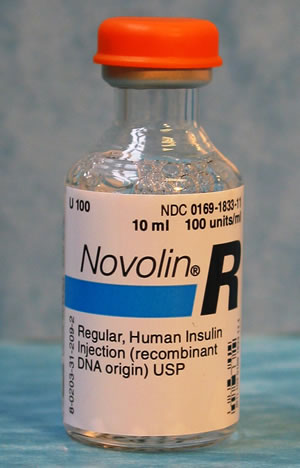
Most nursing units only have one ADM, which is stationary. Nurses often improvise to save time and steps by using portable carts instead of making trips back and forth from the bedside to the ADM. This is an efficient (and understandable) solution from their perspective, but it also represents a workaround that bypasses the safety features built into the ADM system. The risk of pulling the wrong medication out of the medication cart is also increased if the patient is receiving look-alike medications, as may have been the case here (Figure 3 and Figure 4) [See related commentary]. Manufacturers should take steps to avoid look-alike vials where possible, and hospital policies should be in place to avoid such errors.
Human Factors
The fact that the nurse had nine patients on a skilled nursing unit probably means that she was extremely busy and hurried and likely susceptible to unanticipated interruptions. When people are in a hurry or their concentration is broken repeatedly, they can easily mistake one item for another, or, when reading a label, not really see the words at all. Even under the best circumstances, there are limits on human thinking and the ability to be consistently accurate. Maintaining one’s attention in the presence of excessive stimulation is sometimes impossible.(1) Delivery of medications involves a complex set of steps, including precise motor skills, primary and working memory, attention, focus, and concentration. In one study, nurses were interrupted approximately six times per hour during their shift, and most interruptions occurred while nurses were performing interventions, particularly medication administration.(3) Clearly, the interval around medication administration is a vulnerable time, both for the nurse and for the patient.
Most health care providers are not educated about human factors issues and the potential influence of these factors on accurate performance of complex tasks. Moreover, health care workers often overestimate their abilities and underestimate their limitations when it comes to medication delivery.(4) It is likely that nurses who are better educated about the importance of human factors in their work will be better able to anticipate and guard against hazardous situations or help redesign them to make them safer.
Workload and Environment
Nurses are being held responsible for care, protection, and safety of an ever-increasing number of patients, in an environment replete with distractions and interruptions. These factors have been shown to increase the occurrence of preventable medication errors.(1) Many of the interruptions involve non-nursing functions and interruptions that require a response. Nurses feel that they must respond to these interruptions and hassles (5), but doing so increases the chance of errors.
In addition to interruptions and hassles, another factor that increases the risks to patients is low nurse-to-patient ratios. One study of ICU patients found that patients exposed to high nurse-to-patient ratios were twice as likely to die as those with lower nurse-to-patient ratios.(6) Addressing this issue is particularly important with the increasing complexity of today’s patients, driven partly by the aging of the population. For example, elderly patients, such as those found on a skilled nursing unit, require much more time and attention. We can no longer assume that any nurse should be able to care for “X” number of patients on any given day.
Because of this, a recent Institute of Medicine (IOM) report recommended that hospitals should scale back the workload of their staff nurses.(7) In addition, the lack of nursing leaders and managers and the scaling back of ranks of nursing managers has reduced direct support of patient-care staff. Nurses should have the authority to stop admissions to their units when they believe that staffing is inadequate. Hospitals should hire more nurses and not use the excuse that there is a shortage. They need to improve nurse retention and make nursing more appealing. Hospitals must include some excess nurse capacity into each shift to provide for unexpected situations. Administrators also should strive to improve the public perception that efficiency and cost containment are more important than patient safety.(7) Not only are appropriate nurse ratios an important factor in patient safety, they also improve nursing satisfaction and decrease the potential for burnout. Hospitals should also replace upper levels of nurse managers so nurses have the support they need.
Recommendations
Despite the nursing shortage, hospital administrators must reduce the workload for nurses and build in extra nursing staff to accommodate emergency situations. Establish nurse-to-patient ratios that are realistic and safe, while allowing nurses the ability to refuse new admissions when they feel it is unsafe to do so. Educate nurses and other staff about human factors and the effect they have on medication errors. Consider the environment in which nurses are working and redesign systems to work for them, not against them. Nurses need more nurse managers and other support staff in light of the heavy patient care needs and technology they face today. If ADMs are used, acquire sufficient numbers so that they can be placed in close proximity to patient rooms. When scheduling nurses, managers should take into consideration the amount of experience each staff member has, the amount of care the patients need, admissions, discharges, and patients moving to a different floor. Consider flexible scheduling for some nurses, especially older nurses, who may not be able to work a 12-hour shift.
Take-Home Points
- All medication orders create an opportunity for error.
- Placing medications from the ADM into another medication cart circumvents the intended safety features.
- More ADMs should be made available in closer proximity to patient rooms.
- Look-alike vials should not be stored in close proximity.
- Distractions and interruptions lead to medication errors; nurses should be allowed sufficient uninterrupted time to administer medications.
- Hospitals should scale back the workload of their staff nurses to achieve safe nurse-to-patient ratios.
Tess Pape, PhD, RN, CNOR Assistant Professor Patty Hanks Shelton School of Nursing A consortium of Abilene Christian, Hardin Simmons, & McMurray Universities, Abilene, TX
References
1. Pape TM. Applying airline safety practices to medication administration. Medsurg Nurs. 2003;12:77-93; quiz 94. [ go to PubMed ]
2. Oren E, Shaffer ER, Guglielmo J. Impact of emerging technologies on medication errors and adverse drug events. Am J Health Syst Pharm. 2003;60:1447-1458. [ go to PubMed ]
3. Potter P, Wolf L, Boxerman S, et al. Understanding the cognitive work of nursing in the acute care environment. J Nurs Adm. 2005;35:327-335. [ go to PubMed ]
4. Schneider PJ. Applying human factors in improving medication-use safety. Am J Health Syst Pharm. 2002;59:1155-1159. [ go to PubMed ]
5. Beaudoin LE, Edgar L. Hassles: their importance to nurses’ quality of work life. Nurs Econ. 2003;21:106-113. [ go to PubMed ]
6. Tarnow-Mordi WO, Hau C, Warden A, Shearer AJ. Hospital mortality in relation to staff workload: a 4-year study in an adult intensive-care unit. Lancet. 2000;356:185-189. [ go to PubMed ]
7. Morrissey J. Quality vs. quantity. IOM report: Hospitals must cut back workload and hours of nurses to maintain patient safety. Mod Healthc. November 10, 2003;33:8, 11. [ go to PubMed ]
Figures
Figure 1. Automated Dispensing Machine

Figure 2. Portable Medication Cart

Figure 3. Zofran Vial
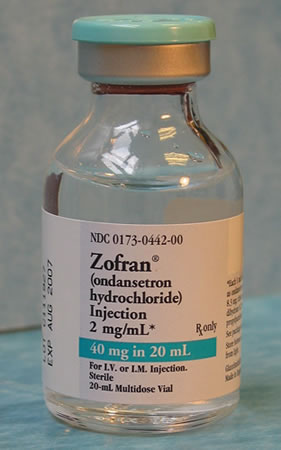
Figure 4. Insulin Vial