The Forgotten Drip
The Case
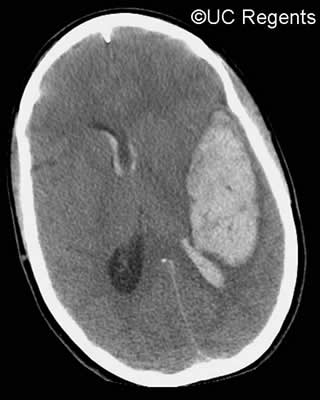
A 45-year-old man was brought to the emergency department by his friends because of a 1-day history of a severe headache and "bizarre behavior." A computed tomography (CT) scan of his brain revealed acute intracranial hemorrhage with cerebral edema, evidence of midline shift, and increased intracranial pressure (Figure). The patient was admitted to the intensive care unit (ICU).
Multiple therapies were initiated to reduce the intracranial pressure and swelling, including intubation and mechanical ventilation, intravenous steroids, and an infusion of mannitol. In addition, intravenous fluids were withheld, to prevent worsening of the cerebral edema. Over the next 24 hours, the patient showed minimal improvement and remained unresponsive and comatose. Repeat CT scanning showed a stable hemorrhage but persistent cerebral edema.
On hospital day 2, another CT scan showed that the hemorrhage was unchanged, but there was significant improvement in the cerebral edema. Based on these results, the physicians expected the patient's mental status to be improved; however, he remained in a coma. A review of that day's laboratory data revealed that the patient had developed severe hypernatremia (high enough to explain his continued altered mental status) and new acute renal failure since admission. Nephrology was consulted to help determine the etiology of the hypernatremia and renal failure and to make recommendations about management.
In reviewing the records, consultants realized that the mannitol infusion had been continued for more than 24 hours at a very high dose. The mannitol, as expected, had induced a profound osmotic diuresis. Because the patient had not received any additional intravenous or enteral fluids, he had become severely dehydrated. Although the hemorrhage and cerebral edema were improved, the patient remained unresponsive and comatose because of the hypernatremia and acute renal failure. He had a prolonged hospitalization and ultimately died from complications related to renal failure.
The Commentary
Spontaneous intracerebral hemorrhage (ICH) is the etiology of 10%–20% of new strokes each year in the United States. It is a tremendously morbid disease, with one third to one half of patients dying within 30 days of their hemorrhage. There are currently no approved therapies specifically targeting ICH, and evidence-based acute management focuses on mitigating the effects of cerebral edema, managing hydrocephalus, controlling hypertension, and preventing hospital-acquired complications.(1)
Elevated intracerebral pressure (ICP) is found in many cases of ICH, and its prompt treatment likely improves outcome. Two general pathophysiologic approaches toward elevated ICP have been touted in the literature. The "Lund protocol," derived in patients with elevated ICP in the setting of head trauma, assumes that the normal blood-brain barrier is disrupted and focuses on procedures designed to maintain fluid within the intravascular compartment in order to avoid increasing brain parenchymal edema.(2) A second, potentially complementary approach is driven by the concept of the cerebral perfusion pressure (CPP, calculated as mean arterial pressure [MAP] – ICP).(3) This CPP-driven strategy emphasizes measures designed to minimize cerebral ischemia by keeping CPP greater than 70 mm Hg, either by lowering ICP or raising MAP. In ICH, this CPP-driven goal must be balanced against the potential danger of hematoma expansion that can result if MAP remains persistently elevated.
Management of increased ICP in patients with ICH should always begin with simple but effective measures including raising the head of the bed to 30 degrees, which decreases ICP by increasing venous return from the brain, and avoidance of hypotonic fluids (solutions with lower tonicity than blood, such as half normal saline [1/2NS] or dextrose in water [D5W]). Isotonic solutions, such as normal saline (NS), should indeed be administered to ICH patients in order to maintain euvolemia. Intravascular hypovolemia can lead to cerebral hypoperfusion and possibly ischemia. Moreover, infusion of isotonic fluid and maintenance of euvolemia can prevent the systemic effects of dehydration that occurred in this case. In addition, adequate sedation and analgesia in ICH patients will prevent spikes in ICP associated with agitation and pain and should be an integral part of initial ICH management.
If ICP remains elevated clinically despite these simple measures, a more aggressive approach is indicated. Although no randomized data exist, many experts recommend placement of an ICP monitor in order to be able to objectively titrate these interventions once a more aggressive approach is warranted. ICP monitoring devices are small plastic catheters that are inserted into the brain to measure ICP. If increased ICP is secondary to hydrocephalus from either intraventricular blood or obstruction of cerebral spinal fluid (CSF) outflow, placing a ventriculostomy in order to reduce ICP via CSF drainage is a must and may be life-saving for some patients. Most ventriculostomy devices also allow for accurate intermittent measurement of ICP in addition to drainage. Classic teaching has suggested that hyperventilation is fundamental in the management of ICP. However, although hyperventilation is a rapidly effective method of reducing ICP, its utility is limited by its very transient effect and simultaneous lowering of cerebral blood flow; as a result, it should be used only on a very temporary basis in patients with elevated ICP.(4)
Osmotic therapy remains the basis of most aggressive ICP management protocols. Mannitol and infusions of hypertonic saline are the most common agents used for this purpose. Mannitol induces a brisk osmotic diuresis since it is not absorbed in the renal tubule and will pull fluid into the urine. Mannitol should almost always be used intermittently in bolus fashion, based on clinical neurologic deterioration or elevations in ICP measurements, rather than via a continuous intravenous drip. In order to avoid renal failure and volume depletion (5,6), a strict institutional protocol should involve monitoring plasma osmolality and serum sodium every 4–6 hours whenever mannitol is used. Mannitol should be withheld if the plasma osmolality exceeds 320 mOsm/kg or if the patient becomes hypernatremic. Dosing should be limited to less than 250 mg/kg every 4 hours to reduce the chances of renal failure.(7) In patients with preexisting oliguric or anuric renal failure, including patients on dialysis, mannitol should be avoided.
In patients whose ICP remains refractory after the initial simple measures outlined above and osmotic therapy, a variety of third-line approaches are used including neuromuscular blockade, barbiturate coma, and induced hypothermia.(1) Rigorous evidence-based comparisons of these third-line techniques do not exist, and therefore institutional and individual preference guides therapy at this point in ICP management.
In this case, intravenous corticosteroids were also used in an attempt to reduce cerebral edema in a patient with ICH. While corticosteroids are likely effective in reducing edema in some settings such as with intracranial neoplasms, they have no role in ICH as proven by randomized trials and should be avoided in this setting as their use may even be associated with worse outcome.(8)
This case brings up several key points regarding the management of elevated ICP in ICH.
- All centers should develop a step-wise protocol that guides the management of elevated ICP in ICH.
- Use of neuromonitoring to objectively assess ICP in a patient whose clinical examination is poor remains useful to gauge the effects of these interventions. By the time osmotic therapy is instituted, most patients should have ICP monitoring in place.
- Ventriculostomy with CSF drainage allows for reduction of ICP as well as ICP monitoring in patients with obstructive hydrocephalus or intraventricular hemorrhage.
- Mannitol should always be used in a bolus fashion and should never be administered without frequent strict monitoring of serum sodium and plasma osmolality in order to prevent the complications that occurred in this case.
S. Andrew Josephson, MD Assistant Clinical Professor of Neurology Director, Neurohospitalist Program
Department of Neurology
University of California, San Francisco
References
1. Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Circulation. 2007;116:e391-e413. [go to PubMed]
2. Lundberg N. Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psychiatr Scand Suppl. 1960;36:1-193. [go to PubMed]
3. Rosner MJ. Introduction to cerebral perfusion pressure management. Neurosurg Clin N Am. 1995;6:761-773. [go to PubMed]
4. Stocchetti N, Maas AI, Chieregato A, van der Plas AA. Hyperventilation in head injury: a review. Chest. 2005;127:1812-1827. [go to PubMed]
5. Gipstein RM, Boyle JD. Hypernatremia complicating prolonged mannitol diuresis. N Engl J Med. 1965;272:1116-1117. [go to PubMed]
6. Aviram A, Pfau A, Czaczkes JW, Ullmann TD. Hyperosmolality with hyponatremia, caused by inappropriate administration of mannitol. Am J Med. 1967;42:648-650. [go to PubMed]
7. Dorman HR, Sondheimer JH, Cadnapaphornchai P. Mannitol-induced acute renal failure. Medicine (Baltimore). 1990;69:153-159. [go to PubMed]
8. Poungvarin N, Bhoopat W, Viriyavejakul A, et al. Effects of dexamethasone in primary supratentorial intracerebral hemorrhage. N Engl J Med. 1987;316:1229-1233. [go to PubMed]
Figure
Figure. Example CT scan (not from this case) showing acute intracranial hemorrhage with cerebral edema, evidence of midline shift, and increased intracranial pressure.