Wrong Turn through Colon: Misplaced PEG
Sorokin R, Conn M. Wrong Turn through Colon: Misplaced PEG. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2012.
Sorokin R, Conn M. Wrong Turn through Colon: Misplaced PEG. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2012.
The Case
An 87-year-old man was admitted for congestive heart failure (CHF) exacerbation. In addition, a past cerebrovascular accident (CVA) with resulting dysphagia required placement of a feeding tube. The feeding tube was a percutaneously placed gastric tube, placed by gastroenterology 1 month before admission.
During hospitalization, the patient tolerated his tube feeds until hospital day 4, when he developed loose stools. The diarrhea progressed with liters of watery stool daily, necessitating placement of a rectal tube. Various stool studies were sent and failed to reveal an etiology. Bulking agents were added to his tube feeds but did not improve the consistency or volume of his stools. The primary team noted a remarkable similarity in appearance between the tube feeds and the stool. During a tube check, it was discovered that the tip of the feeding tube was in the colon and not the stomach.
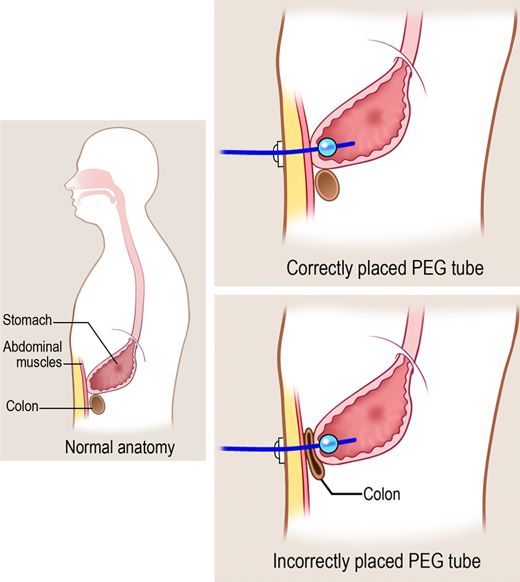
On further investigation, it was determined that a loop of colon was overlying the stomach when the tube was placed. Consequently, while entering the stomach, the gastroenterologists inadvertently passed through the colon. Over time, a fistula formed between the stomach and the adjacent bowel (through which the tube passed during insertion); ultimately, the tube migrated back into the colon, which meant that the feedings were bypassing the entire digestive apparatus of the small intestine.
After the error was recognized, another tube was placed in the stomach and the previously placed tube was removed. However, the delay in identifying the problem resulted in sustained inadequate nutrition and significant decompensation.
The Commentary
The patient in this case was receiving feeding via a percutaneous endoscopic gastrostomy (PEG) tube. More than 200,000 PEGs are placed annually in the United States (1), and enteral nutrition is the mainstay of nutritional support for many chronically and critically ill patients. Enteral nutrition is safer than parenteral nutrition in critically ill adult patients.(2) Nasoenteric feeding tubes provide short-term (less than 4 weeks) enteral nutrition; percutaneous tubes provide feeding directly into the stomach or jejunum when nutritional support is required for more than 4 weeks.(3-6) Compared with nasogastric tubes, PEGs are better tolerated and associated with comparable morbidity.(7)
The goal of PEG insertion is to improve nutritional status, quality of life, and life expectancy.(3,8) The two most common disease states necessitating PEGs are dysphagia secondary to neurologic disorders and head and neck and esophageal cancer undergoing radiation and chemotherapy (Table 1). The use of enteral feeding in severe dementia or in patients with short life expectancies is controversial.(3,8) A PEG should not be inserted as a symbolic gesture or in patients with terminal disease.(3)
Stroke-induced dysphagia precipitated this 87-year-old patient's PEG, a well-recognized indication. His cognitive capacity, long-term prognosis, and quality of life are not discussed. However, such an assessment must be part of the pre-procedure patient evaluation.(9) Some institutions utilize guidelines toward the proper selection of PEG patients.(9)
Absolute and relative contraindications for PEG are listed in Table 2. Although some consider obstruction of the oropharynx, obstruction of the upper gastrointestinal tract and previous abdominal surgery as contraindications (4), others do not.(3) In general, coagulopathies should be corrected prior to insertion of a PEG tube.(10) Because a PEG is inserted under moderate sedation, such patients must be able to tolerate the sedation and endoscopy.
The procedure is performed as part of a standard upper endoscopy.(11) A second physician or a trained assistant performs the abdominal wall portion of the procedure. Many recommend a single dose of a prophylactic antibiotic 30 minutes prior to PEG insertion.(4,12) First, a complete diagnostic endoscopy excludes any abnormalities that would preclude PEG placement. Then, the stomach is insufflated with air, the room lights are dimmed, and the transilluminated endoscope light is identified through the abdominal wall. The second physician compresses the abdominal wall with a single finger at the sharpest point of transillumination and the impression made by the finger is confirmed endoscopically as a good location for tube placement. The second physician sterilely prepares the abdominal wall and anesthetizes the skin. Then, the lidocaine-filled needle is inserted through the abdominal wall into the stomach while it is continually aspirated. Simultaneous air return in the syringe and endoscopic visualization of the needle should be confirmed. This "Safe Tract" technique helps avoid tube placement through an overlying loop of bowel.(13) Aspirated air in the syringe prior to endoscopic visualization of the needle suggests inadvertent insertion into an overlying loop of bowel. In that case, the needle should be removed and reinserted at a slightly different angle, once again utilizing the Safe Tract technique. These four safety procedures (Table 3) minimize inadvertent insertion of the PEG tube through intervening colon.(12,14) In addition, placing the patient in the reverse Trendelenburg position allows gravity to lower any overlying bowel; some clinicians use this technique to further reduce risk.
Once the safe track is confirmed, a trocar is inserted through a small abdominal skin incision into the stomach. A suture or guidewire is passed through the trocar and grasped endoscopically with a snare and withdrawn with the endoscope, leaving a portion still protruding externally at the abdominal wall incision site. With the pull technique, the gastrostomy tube is affixed to the suture and "pulled" back through the esophagus, stomach, and abdominal wall. A soft mushroom-shaped internal bumper and a smaller external bumper holds the tube in place (Figure). With the push technique, the gastrostomy tube is pushed over the guidewire and held in place in similar fashion. Historically, endoscopists have delayed feeding for 24 hours after PEG placement, however earlier feeding after only 4 hours is safe.
PEG remains a remarkably well-tolerated procedure. Procedural-related mortality has been reported to be 0 in a review of 1041 patients.(11) Thirty-day mortality ranges from 5.8% (11) to 6.5% (6,15) and is predicted by older age, low body mass index (BMI), and diabetes.(15) Patients with cancer or malnutrition are associated with increased mortality with PEGs.(9) Complications occur in 8%–30% of PEGs and are categorized as minor or major (9-12,16) and early (≤ 72 hours) or late (> 72 hours).(10) Minor complications include tube clogging, superficial wound infection, and leakage. Nearly 50% of patients experience pneumoperitoneum, which does not usually represent an intra-abdominal catastrophe.(10,12) Major complications include aspiration, inadvertent PEG removal, cancer metastasis at the PEG insertion site, hemorrhage, peritonitis, buried bumper syndrome, gastrocolocutaneous fistula, small bowel injury, gastric outlet obstruction, and necrotizing fasciitis.(12)
This patient had an uncommon, but well described PEG complication: placement of the PEG tube through the colon leading to a gastrocolocutaneous fistula.(14) This complication occurs when the PEG tube traverses the colon during insertion, presumably because the colon is between the stomach and abdominal wall at that time. In a review of 28 such cases, 16 occurred after PEG replacement; thus, it is important to follow standard safety practices during PEG replacement, despite presumably mature PEG tract.(14) Similar to this patient, half of these patients with misplaced PEGs presented with symptoms of severe watery or white colored diarrhea; the others developed fecal material in the PEG tube or around the PEG tube site.(14)
Diarrhea is observed in 10%–20% of PEG patients and may reflect hyperosmolar solutions, medications such as antibiotics or antacids, infection, lactose intolerance, or fat malabsorption.(12) As this case illustrates, post-PEG diarrhea mandates prompt and thorough evaluation. Unresolved diarrhea should spark consideration of a gastrocolocutaneous fistula. A contrast radiograph through the PEG tube (fistulogram) confirms the diagnosis. Usual management consists of simply removing the tube and allowing the fistula to close. Surgery is required rarely with the development of peritonitis or failure of fistula closure.(14)
Post-procedure care involves avoiding tight traction on the PEG tube as this practice may increase ischemia and delay wound healing.(3) All dressing changes should incorporate a careful wound inspection for redness or leakage. Overall, prevention of PEG complications requires careful patient selection, adherence to standard technical safety procedures, and proper post-procedural care, especially while the PEG tract matures. Adherence to these principles will ensure the safe, effective placement of PEG tubes.
Take-Home Points
- PEGs are indicated to improve long-term nutrition and quality and duration of life.
- Four insertion techniques reduce the risk of PEG insertion.
- Post-PEG diarrhea requires evaluation, and, if not ameliorated, consider rare events, such as PEG misplacement and fistula formation.
Rachel Sorokin, MD Chief Patient Safety and Quality Officer Thomas Jefferson University Hospital
Mitchell Conn, MD, MBA Clinical Associate Professor Thomas Jefferson University
References
1. Gauderer MW. Twenty years of percutaneous endoscopic gastrostomy: origin and evolution of a concept and its expanded applications. Gastrointest Endosc. 1999;50:879-883. [go to PubMed]
2. Heyland DK, Dhaliwal R, Drover JW, Gramlich L, Dodek P; Canadian Critical Care Clinical Practice Guidelines Committee. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN J Parenter Enteral Nutr. 2003;27:355-373. [go to PubMed]
3. Löser C, Aschl G, Hébuterne X, et al. ESPEN guidelines on artificial enteral nutrition—percutaneous endoscopic gastrostomy (PEG). Clin Nutr. 2005;24:848-861. [go to PubMed]
4. Byrne KR, Fang JC. Endoscopic placement of enteral feeding catheters. Curr Opin Gastroenterol. 2006;22:546-550. [go to PubMed]
5. Jain R, Maple JT, Anderson MA, et al; ASGE Standards of Practice Committee. The role of endoscopy in enteral feeding. Gastrointest Endosc. 2011;74:7-12. [go to PubMed]
6. Figueiredo FAF, da Costa MC, Pelosi AD, Martins RN, Machado L, Francioni E. Predicting outcomes and complications of percutaneous endoscopic gastrostomy. Endoscopy. 2007;39:333-338. [go to PubMed]
7. Gomes CAR Jr., Lustosa SAS, Matos D, Andriolo RB, Waisberg DR, Waisberg J. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2010;11:CD008096. [go to PubMed]
8. Freeman C, Ricevuto A, DeLegge MH. Enteral nutrition in patients with dementia and stroke. Curr Opin Gastroenterol. 2010;26:156-159. [go to PubMed]
9. Schurink CAM, Tuynman H, Scholten P, et al. Percutaneous endoscopic gastrostomy: complications and suggestions to avoid them. Eur J Gastroenterol Hepatol. 2001;13:819-823. [go to PubMed]
10. Kurien M, McAlindon ME, Westaby D, Sanders DS. Percutaneous endoscopic gastrostomy (PEG) feeding. BMJ. 2010;340:c2414. [go to PubMed]
11. Richter-Schrag HJ, Richter S, Ruthmann O, Olschewski M, Hopt UT, Fischer A. Risk factors and complications following percutaneous endoscopic gastrostomy: a case series of 1041 patient. Can J Gastroenterol. 2011;25:201-206. [go to PubMed]
12. Schrag SP, Sharma R, Jaik NP, et al. Complications related to percutaneous endoscopic gastrostomy (PEG) tubes. A comprehensive clinical review. J Gastrointestin Liver Dis. 2007;16:407-418. [go to PubMed]
13. Foutch PG, Talbert GA, Waring JP, Sanowski RA. Percutaneous endoscopic gastrostomy in patients with prior abdominal surgery: virtues of the safe tract. Am J Gastroenterol. 1988;83:147-150. [go to PubMed]
14. Friedmann R, Feldman H, Sonnenblick M. Misplacement of percutaneously inserted gastrostomy tube into the colon: report of 6 cases and review of the literature. JPEN J Parenter Enteral Nutr. 2007;31:469-476. [go to PubMed]
15. Zopf Y, Maiss J, Konturek P, Rabe C, Hahn EG, Schwab D. Predictive factors of mortality after PEG insertion: guidance for clinical practice. JPEN J Parenter Enteral Nutr. 2011;35:50-55. [go to PubMed]
16. Potack JZ, Chokhavatia S. Complications of and controversies associated with percutaneous endoscopic gastrostomy: report of a case and literature review. Medscape J Med. 2008;10:142. [go to PubMed]
Tables
Table 1. PEG Indications.(3)
| Indications for PEG |
|---|
| • Cancer: head and neck, gastrointestinal |
| • Neurologic dysphagia: stroke, Parkinson disease, central nervous system tumor, amyotrophic lateral sclerosis, cerebral palsy |
| • Severe trauma |
| • Human immunodeficiency virus / acquired immunodeficiency syndrome |
| • Short bowel syndrome |
| • Prolonged coma |
Table 2. PEG Contraindications.
| Contraindications to PEG |
|---|
| • Hemodynamic instability |
| • Interposed organs between abdominal wall and stomach |
| • Inability to transilluminate the abdominal wall and oppose the anterior gastric wall |
| • Perforated viscus |
| • Severe coagulopathy |
| • Pharyngeal or esophageal obstruction |
| • Peritoneal carcinomatosis |
| Relative Contraindications to PEG |
| • Coagulopathy |
| • Abnormalities of the abdominal wall |
| • Prior gastric surgery |
| • Ascites |
| • Chronic ambulatory peritoneal dialysis |
| • Gastrointestinal tract obstruction |
| • Morbid obesity |
| • Hepatomegaly |
Table 3. PEG Insertion Safety Procedures.
| Four PEG Insertion Safety Procedures |
|---|
| 1. Insufflate stomach |
| 2. Illuminate abdominal wall from endoscope |
| 3. Invaginate gastric wall, visible from endoscope with external digital pressure |
| 4. Aspirate syringe of anesthetic needle to ensure no air return prior to gastric entry, while identifying track for guidewire |
Figure
Figure. Correct and incorrect placement of PEG tube. (Illustration © 2012 by Chris Gralapp.)