Medication Reconciliation With a Twist (or Dare We Say, a Patch?)
Kwan JL. Medication Reconciliation With a Twist (or Dare We Say, a Patch?). PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2014.
Kwan JL. Medication Reconciliation With a Twist (or Dare We Say, a Patch?). PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2014.
Case Objectives
- Appreciate that medication discrepancies are common across the care continuum
- Define the Best Possible Medication History (BPMH) and how to optimally obtain it
- Understand that transdermal patches have a heightened propensity for error
- List different approaches for improving medication reconciliation
- Describe the overall evidence supporting medication reconciliation
The Case
An 80-year-old woman with a history of dementia was admitted to the hospital with abdominal pain and diagnosed with a bowel obstruction, secondary to a new diagnosis of colon cancer. She underwent an uncomplicated surgical resection of the colon cancer with relief of the obstruction. Postoperatively she developed confusion and agitation consistent with acute delirium.
At this hospital, a geriatric psychiatry consulting service was available to help manage postoperative delirium and was consulted by the surgical service. As part of their evaluation, they reviewed the patient's current and prior medications to determine possible triggers and optimize treatment. They spoke directly with the family and reviewed the official medication reconciliation list, which a pharmacist had documented at admission. Although the family stated that the patient was on a "memory medicine," the reconciliation list did not include any dementia medication. Based on this discrepancy, the consulting service contacted the outpatient pharmacy and learned the patient was prescribed a cholinesterase inhibitor patch (a medication for dementia), to be replaced weekly. She had not been prescribed the drug during the hospital stay, and the last patch had been placed more than a week earlier. Although many factors likely contributed to postoperative delirium, the geriatrics service felt that abrupt withdrawal of the cholinesterase inhibitor contributed to the episode.
The Commentary
Transitions of care, such as admission to, transfer within, and discharge from the hospital, are vulnerable periods due to poor communication and inadvertent information loss.(1,2) Unintentional changes to patients' medication regimens represent one important category of such errors.(3-5) Medication regimens over the course of a hospital admission often differ from preadmission medication lists. Discrepancies between these lists may reflect deliberate changes made by the care team related to the hospitalization (for example, withholding antihypertensive drugs from patients in shock); however, they may also be inadvertent and result from incomplete or inaccurate communication and information transfer.
Two common categories of unintentional discrepancies with the potential to cause patient harm are errors of "omission"—medications that are inappropriately not started or continued—and errors of "commission"—medications that patients have discontinued and are inappropriately restarted.(6) Up to 67% of patients have inadvertent drug discrepancies during admission to the hospital (6), with many of these discrepancies persisting at discharge.(4) Fortunately, however, a recent systematic review reported that most unintended discrepancies are not clinically significant; in fact, most patients experience no discrepancies with the potential to cause harm.(7) Thus, although it seems clinically significant discrepancies are unusual, unintentional medication discrepancies are still very common and have the potential to adversely affect patients.
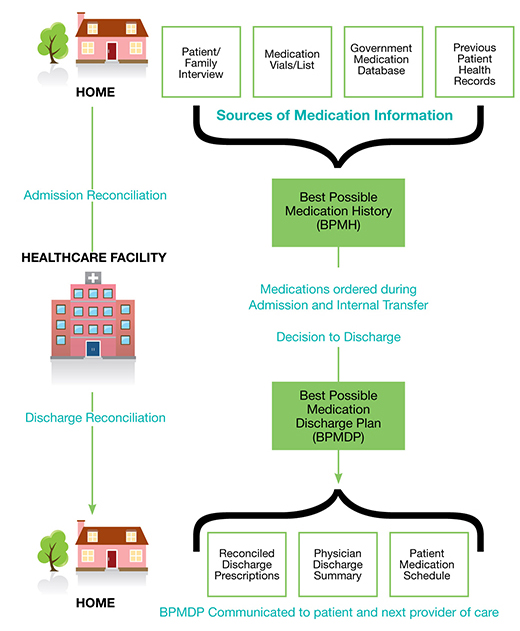
Medication reconciliation is the formal process for identifying and correcting unintentional medication discrepancies across transitions of care (Figure). Medication reconciliation has been previously reviewed in AHRQ WebM&M in multiple cases.(8-10) Since the last case was presented in 2010, there has been significant research and real-world experience in medication reconciliation from which we have developed a much more sophisticated understanding of challenges and best practices.
One point that has become clear is that the best possible medication history (BPMH) is the cornerstone for the "med rec" process. The BPMH is more comprehensive than a routine medication history and involves two steps: (i) a systematic process for obtaining a thorough history of all prescribed and non-prescribed medicines by using a structured patient and/or family interview and (ii) verification of this information with at least one other reliable resource (for example, drug vials, patient medication lists, a community pharmacy, a primary care physician, or a government medication database).(11) At a minimum, medication reconciliation now must include completion of BPMH and the correction of any unintentional discrepancies between a patient's previous medication regimen and the proposed drug orders at admission to the hospital, inpatient transfer between services or units, or hospital discharge. Although physicians are aware of the importance of this process conceptually (12), there are many barriers and challenges that individuals and institutions face that often prevent robust medication reconciliation from occurring.
In the presented case, despite completion of an official medication reconciliation by a pharmacist during a care transition, the cholinesterase patch was omitted from the patient's admission medication list. This omission contributed to preventable harm. Transdermal patches are a route of administration for many different pharmacologic agents including opiates, hormonal therapy, nicotine, and cholinesterase inhibitors. While often convenient, transdermal patches have a heightened propensity for error due to inconsistencies in dosing intervals, in addition to patch design, placement, and identification.(13) A full discussion of the risks associated with transdermal patches is beyond the scope of this commentary, but a description can be found in an FDA Safety Page.(13)
This case serves as an excellent reminder to always include transdermal medications in structured medication interviews, as they can be easily omitted. It also highlights the importance of not "going through the motions" when completing a routine medication history at transitions of care, but rather building a thorough BPMH using a structured patient and/or family interview, followed by verification of this medication list with at least one other source of information. The BPMH was eventually determined by the geriatrics consulting team in collaboration with the outpatient pharmacist.
There are multiple approaches to performing robust, thorough, and accurate medication reconciliation during transitions in care. Enhanced medication reconciliation can involve interprofessional collaboration (for example, pharmacists, physicians, and/or nurses conducting medication reconciliation as a team), integration of the medication reconciliation process into discharge summaries, and combining it with drug counseling to patients.(14) Medication reconciliation has also been bundled with other interventions to improve care transitions at discharge, such as individualized counseling, coordination of follow-up appointments, post-discharge telephone calls, and involvement of a care coordinator or nurse discharge advocate.(15-17) Although most medication reconciliation efforts have centered on inpatient care, there are emerging studies evaluating its efficacy in the ambulatory setting.(18,19) Systematic reviews suggest that medication reconciliation reduces clinically significant medication discrepancies, as well as potential and confirmed adverse drug events. Moreover, while medication reconciliation alone probably does not reduce post-discharge hospital utilization, it may do so when bundled with interventions aimed at improving care transitions.(7,20)
Medication reconciliation has been widely embraced as an important patient safety strategy worldwide. In 2006, the World Health Organization prioritized it as one its top five patient safety goals.(11) National campaigns championing the reduction in preventable adverse events, such as the Institute for Healthcare Improvement's "100,000 Lives Campaign" in the United States (21) and the Canadian Patient Safety Institute's "Safer Healthcare Now!" (22), included medication reconciliation in their core strategies. In 2005, The Joint Commission identified medication reconciliation as one of its National Patient Safety Goals for hospital accreditation. However, due to concerns over challenges with implementation, a modified and more attainable goal was released in 2011 to "maintain and communicate accurate patient medication information" across different points of care.(23)
Pharmacists, who have been shown to play an important role in the prevention of adverse drug events, have become integral to the execution of high-quality medication reconciliation.(7,20,24) However, relying on pharmacists, who are in short demand in most settings, may not be a viable solution. Pharmacists are frequently tasked with the responsibility to safely provide drugs to hospitalized patients. As such, they may find it impossible to complete medication reconciliation, which can be resource intensive, at every transition of care for every patient. This has prompted the development of selection criteria for high-risk patients who would theoretically benefit the most from a comprehensive medication review. These criteria most commonly include older patients, polypharmacy, and/or having more than three comorbid conditions.(20) Currently, the evidence to support the association between such selection criteria for high-risk patients and the reduction in clinically significant discrepancies is mixed.(7,20) Nevertheless, these criteria may provide a starting point for institutions to determine which patients would most benefit from more robust medication reconciliation. However, this case does provide a cautionary note: although this patient was likely identified as high-risk (based on age) and had medication reconciliation performed by a pharmacist, an error still occurred.
Health information technology (IT) has been lauded as a potential solution for the challenges encountered with implementation of efficient and effective medication reconciliation. In a consensus statement issued by the Society of Hospital Medicine, an integrated and easily transferable personal health record was highlighted as being a key principle for making inpatient medication reconciliation patient-centered, clinically relevant, and implementable.(25) The white paper further recommends that, to be implemented effectively, the record must be compatible across all settings and that all health care organizations, pharmacy systems, and insurers must make medication reconciliation–related interoperability and accessibility a priority. In the United States, compatibility has been incentivized by the American Recovery and Reinvestment Act of 2009, which included medication reconciliation among the objectives of the Meaningful Use program.(26) In addition to personal health records, IT has been utilized in many other ways to improve the medication reconciliation process, from simply tracking medications across sites of care to enabling an active comparison of medicines and clarification of discrepancies.(27) These IT interventions have shown variable effectiveness in improving medication reconciliation. In one study, Radley and colleagues report that processing a prescription drug order through a computerized physician order entry system decreases the likelihood of error on that order by 48%.(28)
Medication reconciliation is a widely recommended patient safety strategy that, while surprisingly difficult to implement effectively, can enhance quality and safety. Future research should focus on determining patient features that more consistently predict unintentional medication discrepancies and building tools that allow institutions to easily identify such at-risk patients. In addition, funding agencies should invest in exploring IT-based interventions.(25) Whether medication reconciliation is a high-value patient safety strategy, one in which the benefits outweigh the costs (financial and otherwise), remains to be seen. To date, such cost-benefit studies have tended to fall on the side of benefit.(29,30) This case illustrates both the capacity for medication reconciliation to identify and correct unintentional medication discrepancies, but also the challenges inherent in implementing this safety practice effectively.
Take-Home Points
- Transitions of care are vulnerable periods due to poor communication and inadvertent information loss. Unintentional changes to patients' medication regimens are a well-documented category of such errors.
- Medication reconciliation is the formal process for identifying and correcting inadvertent medication discrepancies across transitions of care.
- Although medication reconciliation has been widely embraced, implementation has been challenging, and its evidence base has been supportive but not definitive.
- Targeting this resource-intensive intervention towards patients with high-risk features, such as older age, polypharmacy, or multimorbidity, may improve its effectiveness.
- Transdermal patches have a heightened propensity for error due to inconsistencies in dosing intervals, in addition to patch design, placement, and identification. It is important that transdermal medications be included in all structured medication interviews.
Janice L. Kwan, MD
Department of Medicine
University of Toronto, Toronto, Canada
Faculty Disclosure: Dr. Kwan has declared that neither she, nor any immediate member of her family, have a financial arrangement or other relationship with the manufacturers of any commercial products discussed in this continuing medical education activity. In addition, the commentary does not include information regarding investigational or off-label use of pharmaceutical products or medical devices.
References
1. Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141:533-536. [go to PubMed]
2. Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA. 2007;297:831-841. [go to PubMed]
3. Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847. [go to PubMed]
4. Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165:1842-1847. [go to PubMed]
5. Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165:424-429. [go to PubMed]
6. Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173:510-515. [go to PubMed]
7. Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):397-403. [go to PubMed]
8. Poon EG. Medication reconciliation: whose job is it? AHRQ WebM&M [serial online]. September 2007. [Available at]
9. Culter TW. Medication reconciliation victory after an avoidable error. AHRQ WebM&M [serial online]. February/March 2009. [Available at]
10. Weber RJ. Medication reconciliation pitfalls. AHRQ WebM&M [serial online]. February 2010. [Available at]
11. High 5s Project. Geneva, Switzerland: World Health Organization; 2013. [Available at]
12. Basey AJ, Krska J, Kennedy TD, Mackridge AJ. Prescribing errors on admission to hospital and their potential impact: a mixed-methods study. BMJ Qual Saf. 2013;23:17-25. [go to PubMed]
13. Transdermal patches: High risk for error? FDA Safety Page. [Available at]
14. Fernandes O. Medication reconciliation in the hospital: what, why, where, when, who and how? Healthc Q. 2012;15:42-49. [go to PubMed]
15. Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4:211-218. [go to PubMed]
16. Kripalani S, Roumie CL, Dalal AK, et al. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157:1-10. [go to PubMed]
17. Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150:178-187. [go to PubMed]
18. Bayoumi I, Howard M, Holbrook AM, Schabort I. Interventions to improve medication reconciliation in primary care. Ann Pharmacother. 2009;43:1667-1675. [go to PubMed]
19. Milone AS, Philbrick AM, Harris IM, Fallert CJ. Medication reconciliation by clinical pharmacists in an outpatient family medicine clinic. J Am Pharm Assoc (2003). 2014;54:181-187. [go to PubMed]
20. Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172:1057-1069. [go to PubMed]
21. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: setting a goal and a deadline for improving health care quality. JAMA. 2006;295:324-327. [go to PubMed]
22. Edmonton, AB, Canada: Canadian Patient Safety Institute. Safer Healthcare Now! Medication Reconciliation. [Available at]
23. Oakbrook Terrace, IL: The Joint Commission. National Patient Safety Goals: Hospital Accreditation Program. January 2014. [Available at]
24. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166:955-964. [go to PubMed]
25. Greenwald JL, Halasyamani L, Greene J, et al. Making inpatient medication reconciliation patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. J Hosp Med. 2010;5:477-485. [go to PubMed]
26. Washington, DC: Office of the National Coordinator for Health Information Technology. Step 5: Achieve Meaningful Use Stage 1. Medication Reconciliation. [Available at]
27. Bassi J, Lau F, Bardal S. Use of information technology in medication reconciliation: a scoping review. Ann Pharmacother. 2010;44:885-897. [go to PubMed]
28. Radley DC, Wasserman MR, Olsho LE, Shoemaker SJ, Spranca MD, Bradshaw B. Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. J Am Med Inform Assoc. 2013;20:470-476. [go to PubMed]
29. Karapinar-Çarkit F, Borgsteede SD, Zoer J, Egberts TC, van den Bemt PM, van Tulder M. Effect of medication reconciliation on medication costs after hospital discharge in relation to hospital pharmacy labor costs. Ann Pharmacother. 2012;46:329-338. [go to PubMed]
30. Karnon J, Campbell F, Czoski-Murray C. Model-based cost-effectiveness analysis of interventions aimed at preventing medication error at hospital admission (medicines reconciliation). J Eval Clin Pract. 2009;15:299-306. [go to PubMed]
31. Fernandes OA. Medication reconciliation: practical tips, strategies and tools for pharmacists. Pharmacy Practice. 2009;25:26.
Figure
Figure. Overview of medication reconciliation through the course of a hospital admission. Reprinted with permission from (31) Pharmacy Practice.